
The objective was to identify latent variables shaping university students’ mental health perceptions and to explore how they view urban environments and preferred interventions. Two sub-objectives (SO) and research questions (RQ) were defined:
SO1 Identify latent components of students’ mental health perception using factor analysis.
SO2 Assess perceptions of urban environment and preferred interventions.
RQ1 What latent components shape students’ mental health perceptions?
RQ2 How do these components reflect awareness and education about mental health?
RQ3 How are urban environment features perceived in relation to mental health?
RQ4 Do gender differences shape perceptions?
RQ5 Which interventions are considered most effective?
Questionnaire and data collection
The questionnaire was developed based on previous research focusing on the prevalence of mental disorders in the population aged 0–25 years in the Czech Republic [10], as well as consultations with experts. It comprised 15 items addressing internal experiences, social background, and institutional conditions. The questionnaire included ordinal (O), nominal (N), and binary (B) variables (see Table 1). It was pilot-tested on a sample of 27 students to ensure clarity and relevance, and was subsequently administered online in February 2025 to students from four major Czech universities in the field of social sciences. According to Czech Statistical Office data, a total of 5,700 students in economics were enrolled in this field at these universities in 2024 [11]. Information about the study was disseminated to students at all institutions via the internal university system Edison and through the official social media channels of the universities, where a link to the Google Forms questionnaire was also provided. In total, 767 valid responses were obtained.
Ethics approval was obtained from the Ethics Committee of VSB-Technical University of Ostrava, reference no. VSB/25/044396. The study was conducted in accordance with the Declaration of Helsinki. All participants provided informed consent prior to participation. Incomplete responses were excluded using listwise deletion, and only cases with valid answers to all relevant items were included in the statistical analysis.
The questions are introduced in Table 1 below.
Table 1 Questions for the quantitative research
The research (including questionnaire design) was grounded in the assumption of a two-factor model, where latent dimensions of mental health perception include both aspects of well-being (e.g., subjective state, support) and threat factors (e.g., loneliness, lack of access to care). The two-factor model [12, 13] conceptualises mental health as two independent yet co-existing domains. The first domain includes psychopathological symptoms and difficulties, while the second comprises psychological functioning and well-being. In line with Bernanke et al. (2017) [14], who applied latent class analysis to identify groups of students with different mental health risks, this study also seeks to uncover hidden patterns in students’ perceptions of their well-being. The methodological approach was further inspired by Zhou et al. (2020) [13], who used latent profile analysis to distinguish different types of adolescent mental health, supporting the value of person-centred approaches for identifying latent patterns in subjective perception.
Analytical strategy
Data were analysed using principal component analysis (PCA). Suitability of the data was confirmed by a Kaiser–Meyer–Olkin measure (KMO = 0.523) and Bartlett’s test of sphericity (χ²(28) = 289.0; p
PCA transforms the original variables X₁, X₂, …, Xₚ into new, orthogonal components Zₖ that maximise variance in the data (1):
$$Z_{k}\;=\;a_{k1} X_{1}\;+\;a_{k2} X_{2}\;+\;\ldots\;+\;a_{kp} X_{p}\;=\;{a_{k}}^{t} X$$
(1)
where aₖ is the eigenvector of correlation matrix Σ. The components are independent of each other and maintain order according to the explained variance.
The number of components retained was determined by the Kaiser criterion (eigenvalue > 1) and the scree plot. To increase interpretability, varimax rotation was applied, which maximises high loadings and minimises low loadings, thereby clarifying the structure of latent dimensions. Reliability was assessed using Cronbach’s alpha.
Although PCA is not equivalent to a latent variable model, its application in this study enabled identification of patterns of perception. The extracted components should therefore be interpreted as exploratory perception patterns rather than validated latent constructs.
Factor scores and statistical testing
Factor scores were calculated as weighted averages of items, with weights corresponding to the factor loadings. To assess gender differences, Welch’s t-test for independent samples was employed, as it does not assume equality of variances. Effect sizes were calculated using Cohen’s d to estimate the magnitude of observed differences.
All statistical analyses were conducted using IBM SPSS Statistics (Version 29).
Results of the questionnaire survey
The online questionnaire was completed by 767 respondents aged 18–26 years. The most frequent ages were 20 (20.7%), 22 (19.8%), and 21 years (18.4%). Women accounted for 60.5% of the sample and men for 39.5%. Regarding place of residence, almost half of respondents reported living in urban areas (46.2%), while 29.9% lived in mixed urban–rural environments and 24.0% in rural areas.
Latent variables: principal component analysis
Principal component analysis (PCA) initially identified three components with eigenvalues greater than 1, explaining 46.9% of the total variance (Table 2; Fig. 1). However, the second component (“Contextual and interpersonal support”) contained only two items (Q9 and Q11) and showed very low internal consistency (Cronbach’s α = 0.285). As this value fell well below the accepted threshold, only two components were retained for interpretation (PC1 and PC3).
Table 2 Total variance explained
Although the three-component solution explained 46.9% of the variance, only PC1 and PC3 were retained. Together, they accounted for 32.2% of the variance (PC1 = 17.9%, PC3 = 14.3%). The scree plot (Fig. 1) illustrates the eigenvalue distribution and confirms the importance of the first three components, with a clear drop after the third.
Fig. 1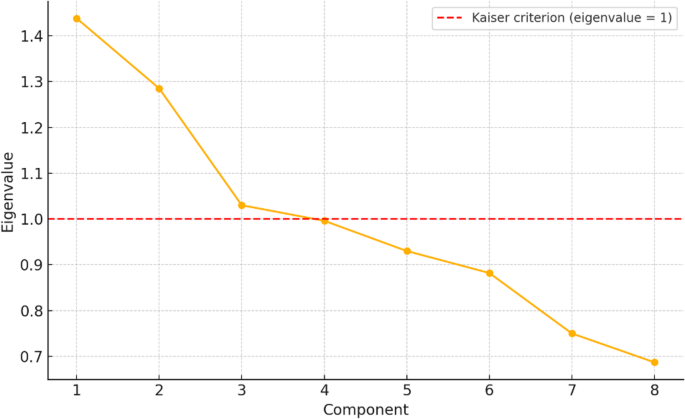
Varimax rotation redistributed the explained variance and highlighted the dominant loadings of the items. Figure 2 presents a heat map of factor loadings, showing contributions of each questionnaire item (Q1–Q15) to PC1 and PC3.
Fig. 2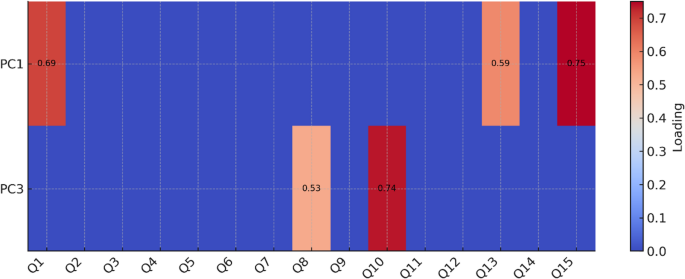
Component 1: Subjective perspective on mental health.
This factor included items relating to individual experiences and self-assessment: loneliness in dealing with mental health (loading = 0.750), evaluation of current mental state (0.693), and perception of mental health awareness in schools (0.590). It can be interpreted as students’ self-perception and awareness of their own mental health.
Component 3: Social and institutional determinants.
This factor grouped items on broader social and institutional aspects: perceived impact of parents’ age on children’s mental health (0.736), preferred place of living in terms of mental health (0.528), and availability of mental health care (0.508). It can be understood as the institutional and community dimension of mental health.
Gender differences
Factor scores were calculated as a weighted average of items using the factor loadings. Welch’s t-test for independent samples was applied. The results showed that for Component PC1, there were no statistically significant differences between men and women (t = − 1.31; p = 0.192; Cohen’s d = − 0.14). For Component PC3, statistically significant gender differences were observed (t = − 3.49; p
Results of the perception of mental health influences and interventions
Which factors do you think affect the mental health of young people aged 18–25 the most?
Figure 3 illustrates the distribution of respondents’ perceptions of external factors influencing mental health, broken down by gender (women N = 464, men N = 303; overall N = 767). Each respondent selected up to three of seven predefined factors perceived as having a negative impact on mental health.
The most common determinant was workload related to study or employment, reported by 78.5% of respondents, with women emphasising this factor more strongly. Social media and technology (66.6%) ranked second, and family relationships (61.0%) third, both more frequently mentioned by women. Loneliness and social isolation were relevant for 57.4% of respondents, again more often among women. About half of the respondents (52.3%) cited economic conditions as a stressor, with no significant gender differences.
By contrast, factors such as crime and feelings of insecurity (4.3%) and lack of access to healthcare (3.9%) were reported only marginally, suggesting lower subjective relevance in relation to mental well-being.
Overall, women more frequently identified stressors connected with the social environment, interpersonal relationships, and digital technologies.
Fig. 3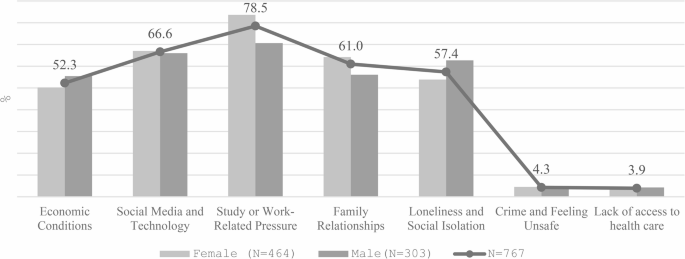
Factors affecting university students’ mental health
Figure 4 shows the frequency of positively perceived aspects of the urban environment. Respondents selected up to three of six predefined factors.
The most significant benefit was the broader social and cultural offer (81.1%), underscoring the role of cities as places of cultural stimulation and social engagement. Access to employment and education (64.8%) ranked second, reflecting the city’s socio-economic opportunities. Wider social contacts (42.1%) and better accessibility of public transport (42.4%) were also reported, with minor gender differences. Easier access to healthcare (37.5%) was more frequently mentioned by women, indicating higher sensitivity to institutional support.
Greater anonymity and privacy were mentioned by only 24.5% of respondents, suggesting low importance of individualisation in this context. Overall, urban environments were primarily valued for cultural, educational, and economic opportunities, while privacy, anonymity, and healthcare availability played a secondary role.
Fig. 4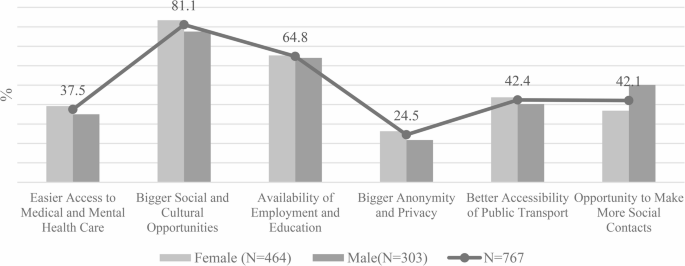
Positive factors City life on mental health
Figure 5 displays perceptions of urban disadvantages. Respondents again selected up to three of six predefined factors.
The most frequent issue was increased stress and fast pace of life (74.2%), more strongly reported by women. Almost as many respondents (72.9%) emphasised the lack of natural environments and quiet areas, confirming the role of nature in psychological well-being. Noise and pollution (62.3%) ranked third, again highlighted by women.
Less frequently mentioned, but still notable, were competitive working environments (30.8%), higher crime rates (26.1%), and anonymity associated with loneliness (23.5%). These factors, although less common, may still significantly affect certain subgroups.
In summary, urban disadvantages were most often associated with stress, environmental deficits, and sensory overload, while crime and social isolation were less prominent.
Fig. 5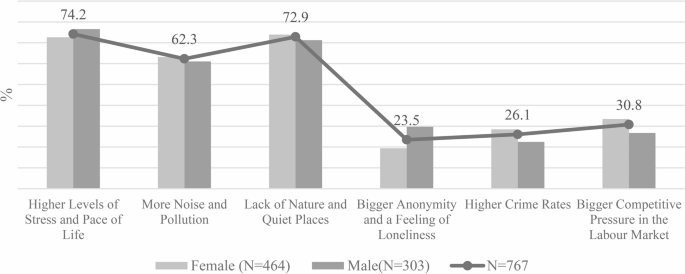
Negative impact of life in the City on mental health
Figure 6 presents the respondents’ preferred areas of improvement in mental health care (five options available).
The most common priority was strengthening support in schools and universities (57.2%), highlighting educational institutions as key points for prevention and early intervention. This was followed by better preventive care systems (44.6%) and improved availability of specialist care (44.5%), both more frequently mentioned by women.
Other relevant areas included reducing financial barriers to care (40.7%) and awareness campaigns (39.2%).
Overall, respondents prioritized systemic changes with an emphasis on prevention, the university environment, and access to specialized care, with gender differences remaining relatively consistent across categories. Similar conclusions were reached by the authors in [15].
Fig. 6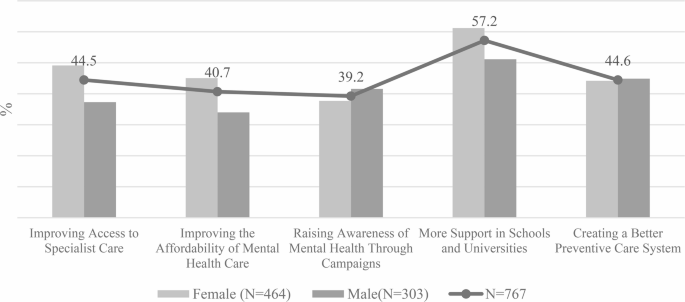
What can improve mental health of young people?