
Study area and study population
Jasikan District has a total population of 59,181, with 37.8% below the age of fifteen. Data from the National Population and Housing Census (2010) depicts a broad base population tapering at the top with 6.7% elderly persons. About 72.4% of the Jasikan population resides outside the district capital, Jasikan. There are five [5] sub-districts, six [6] health centres, fourteen [14] community-based health planning services (CHPS), one [1] private health facility, thirteen [13] faith healers, three [3] traditional/herbal practitioners, one [1] pharmacy and forty-five (45) over-the-counter-medicine-sellers (OTCMS) (Fig. 1).
Fig. 1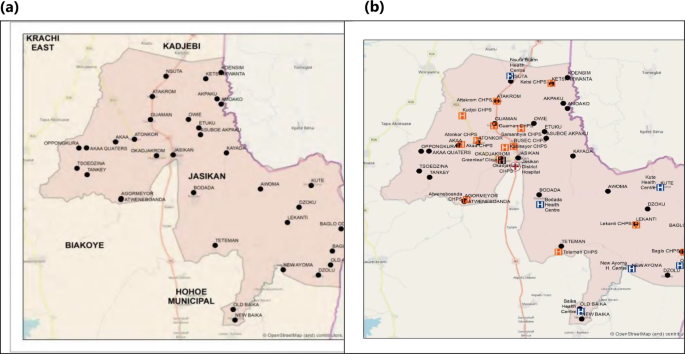
Focused map showing the study area, (a) distribution of communities included in the study, and (b) distribution of healthcare facilities overlaid on the communities included
The majority of the workforce in the municipality is employed in agriculture, which drives the majority of its economic activity. Cocoa and coffee are significant crops besides food crops including yams, cassava, and maize. Along with timber harvesting, urban areas also see growth in the retail and services sectors. In the Jasikan Municipality, Lelemi, Twi, and Ewe are the most often spoken languages. 77% of people aged 11 and above are literate, while 23% are not. Male literacy rates are higher (84.2%) than female literacy rates (70.2%). Six out of every ten persons (60.6%) in the district could read and write both in English and in a Ghanaian language (Ghana Statistical Service, 2014).
Theoretical framework
The theoretical framework used in this study is illustrated below (Fig. 2).
Fig. 2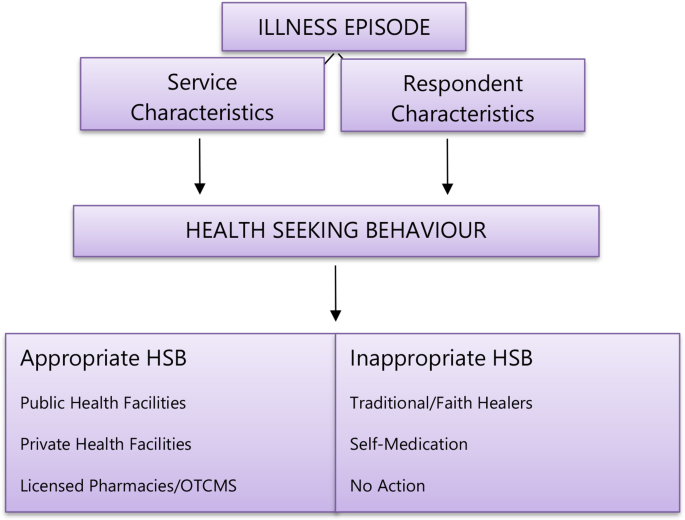
Theoretical framework for the research: In this framework, during an episode of illness, an individual’s health-seeking behaviour is influenced by service characteristics and personal characteristics. Service characteristics include whether it is public or private, proximity, perceived quality of care the facility provides, availability of resources, etc. Individual characteristics also include insurance status, income level, etc. Traditional healers being referred to in this study do not include trained herbal medicine practitioners
The research carried out in the Jasikan District focused on a set of interconnected goals. Initially, the study sought to identify the primary healthcare facility people in the Jasikan District turn to and examine the socio-demographic factors influencing their choice. The study also delved into the factors affecting the healthcare-seeking behaviour prevalent among the local population. Furthermore, an essential aspect of our research objectives was to assess the significance of well-being clinics in influencing healthcare-seeking behaviour. These objectives collectively contribute to the overall analysis of healthcare engagement in the Jasikan District.
Definition of outcome variablesAppropriate health-seeking behaviour
Seeking health care at public health facilities, private health facilities, and licensed Pharmacies/OTCMS regulated under the Health Professions Regulatory Bodies Act 2013, ACT 857, and Health Facilities Regulatory Agency (HeFRA) which was established by the Health Institutions Act 2011, Act 829.
Inappropriate health-seeking behaviour
Seeking health care at traditional/faith healers, engaging in self-medication, and not taking action during an illness episode.
Study design
The study was a community-based cross-sectional study using a mixed method of data collection (Appendix 1.1). We included participants who were ≥ 18 years old, were residents of Jasikan, and had sought healthcare in the last month. Informed consent was obtained from all participants who partook in this study.
Sample size and data collection
The Raosoft sample size online calculator (http://www.raosoft.com/samplesize.html) was used to estimate a minimum representative sample size for this study to achieve stronger statistical power. This method has become very popular in estimating sample sizes since it has been known to produce results similar to that of G-power [19]. For a population of 59,181 in Jasikan District (Ghana Statistical Service, 2014), 5% margin of error, 95% confidence interval, and a response distribution of 50%, the Raosoft calculator estimated a minimum sample size of 382.
A simple random sampling technique was used in data collection from participants. The sample was calculated by a proportionate stratified sampling of respondents from each of the five [5] sub-districts, considering the population of only the 20 largest communities as recorded in the 2010 National Population Census (Ghana Statistical Service, 2014).
The 2010 National Population Census data, released in 2014, was used because the more recent census data were unavailable during data collection.
Data was collected from the 20 largest communities in the district because it adequately represents a homogenous and dynamic mix of residents. Smaller communities are mostly clusters of families residing close to their farms. These settler communities tend to possess similar behavioural characteristics akin to the family head or traditional leader. Since a good mix of individuals of varied educational, economic, traditional, cultural, and religious backgrounds is needed to represent the behaviour of the people of Jasikan District, data was collected from the 20 most populated communities. Moreover, smaller communities may not have access to health resources compared to the other populated communities. This reduces bias and skewness of patterns of health-seeking in smaller communities.
Hence, data was collected from the 20 most populated communities within the municipality. The estimated population of the twenty largest communities sampled is 45,843; therefore, the working sample was stratified to 295, as shown in Table 1 below. The following equation determined the strata sample size:
$$\:{n}_{h}=\:\frac{{N}_{h}}{N}\:n$$
where nh is the sample size for stratum h, Nh is the population size for stratum h, N is the total population size, and n is the total sample size.
Data was collected from consented respondents, using a semi-structured questionnaire, at a single time point from participants in the target population. The questionnaire was hosted and administered to respondents using a web-based data collection tool, KoboCollect Toolbox, part of an open-source KoboCollect Toolbox suite (https://www.kobotoolbox.org/).
Table 1 Population of the twenty largest communities in Jasikan District from which stratified samples were derivedStatistical analysis
Frequency tables were used to summarise data from the socio-demographic and clinical characteristics of patients included in this study. Percentages were calculated for discrete or categorical data, while Mean ± Standard Deviation was generated for continuous variables. Cramer’s V was used to measure the significance and effect size between categorical variables.
The degree of agreement with a statement concerning health-seeking behaviour was recorded on a five-point Likert (ordinal) scale and analysed by summarizing frequencies and categorising responses into excellent/high quality, good/acceptable and poor/improvement required, as documented by Rubaish (2011).
In our investigation into the relationship between demographic characteristics and the appropriateness of health seeking behaviour, we utilized a simple binary logistic regression model using a stepwise forward model. The model was designed to predict the binary outcome of heath seeking behaviour — 1 for appropriate HSB and 0 for inappropriate HSB — based on the independent variables that were identified to have significant association to HSB in the Cramer’s V association tests; age ( 30 years = 1), sex (female = 0, Male = 1), religion (other religion = 0, Christianity = 0) and insurance status (not insured = 0, not insured = 1).
Statistical analyses were performed using the SPSS Statistics 25 (IBM, USA) and SigmaPlot® version 12.5 for Windows (Systat Software Inc. USA). In all the analyses, a p-value less than 0.05 was considered significant.