
They met on the dance floor of a Bolivian bar: a Brooklyn boy named Bill and the girl soon to be known as Marina Brown, twirling together toward a first child and a wedding blessed by the U.S. Peace Corps. Later, Bill Brown became a production man, holding factory management jobs that took their growing family from Mexico to Kuala Lumpur. They raised four children. Marina got a master’s in social work, aiding Miami’s troubled youths. Growing older, the Browns settled in Hawaii but bought another home in Portland, where two of their kids had taken root.
These are the memories. What happened next no one foresaw. Little by little, Marina began to change. She grew dizzy, fainted, got tingles in her arms. Her heart sometimes raced. Doctors doctored. “The medical workup was always negative,” says her son Nick. “There was nothing they could find.”
The ailment ran deep. Marina cried often—sudden outbursts before returning to normal. She asked anxiously about her grandchildren and grew agitated, despondent, paranoid, impulsive. As a passenger in a moving car, she grabbed the steering wheel. She tried to run from the house—and, later, the hospital. She was pushing 83, and could seem forgetful, but tests ruled out dementia. For long periods, she barely talked at all.
Nick is a child psychiatrist and his sister Benjamina a family medicine doctor, yet this was all not just upsetting but perplexing. Looking back, Nick reflects that his mom’s life always revolved around family, and the family was moving away. “She’s always been very kindhearted,” he says, “but she’s not one to necessarily talk about how she feels easily. I think that got in the way of seeing what was really going on.”
Then they saw it. And the family embarked on a maddening quest to get Marina a relatively simple treatment that no one around Portland could, or would, provide.
Nick was recounting much of this in quiet tones before pulling in beside a yellow corner house off Southeast Sellwood Boulevard overlooking the Willamette River, which could be seen dimly through a heavy morning mist. Bill answered the door, leaning into a slight hunch. Behind him was a well-appointed home loaded with the eclectic artistic spoils of a globe-trotting life. A young woman stood farther back—from the nursing agency.
And there was Marina, wobbly, small, rigid, and very, very distant. Nick approached his mother. He spoke slowly. “Hi, Mama,” he said, “it’s me.”
After a series of dead ends, about eight months ago clinicians found a diagnosis for Marina: catatonia, a mysterious psychiatric disorder tied to major, rapid onset depression. But efforts to shake her from this state—psychotherapy, benzodiazepines—have shown little impact.
There is another treatment. It carries a stigma, in which Oregon plays a key role. For many, it does nothing, and it’s not without side effects. But for some with severe psychiatric illness, including the catatonic, it has been known to have profound effects—jolting the psychotic and mute back to the person they were before.
“It’s the closest psychiatry gets to the laying of hands,” says Dr. Harold Sackeim, founding editor of Brain Stimulation, a scientific journal. “It feels miraculous in many ways.”
The treatment is electroconvulsive therapy. ECT is the modern, tamer version of what was once known as electroshock therapy, and the idea is to cause seizures. Theories vary as to why it works but, even as promising new neural stimulation treatments come online, many researchers believe ECT remains today the most effective remedy for treatment-resistant depression.
It is not particularly complex to administer. Yet remarkably few clinicians take up the trade—and not, says Dr. Mohamad Matout of Stanford Health Care, because of any great disagreement about the evidence.
“ECT,” Matout says, “is often approached with a reserve that cannot be explained rationally.”
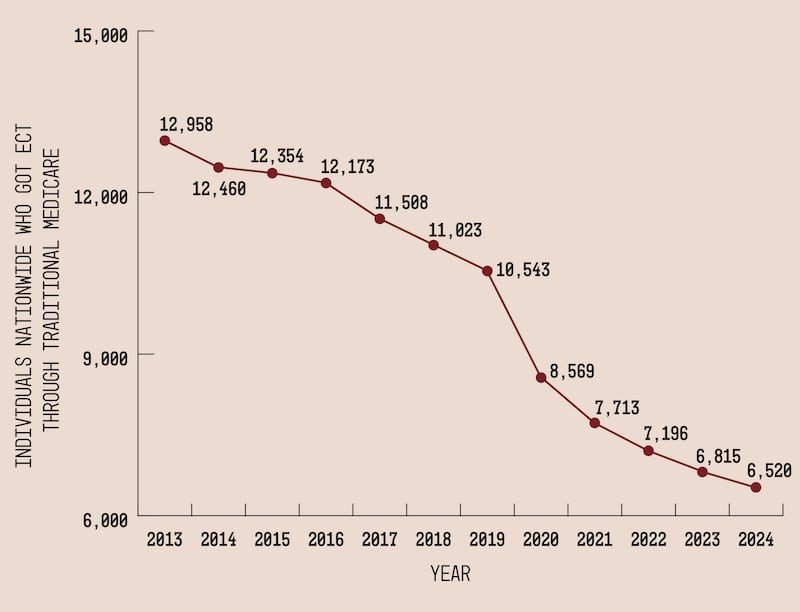
Between 2013 and 2024, an WW analysis has found, ECT services billed to Medicare nationwide declined by half.
 Oregon’s “All Payer All Claims” database documents most ECT treatments in the state, including those billed to Medicaid, commercial insurance, and Medicare Advantage. It documents 109 unique people who received ECT in 2024—slightly fewer than in most previous years.
Oregon’s “All Payer All Claims” database documents most ECT treatments in the state, including those billed to Medicaid, commercial insurance, and Medicare Advantage. It documents 109 unique people who received ECT in 2024—slightly fewer than in most previous years.
Meanwhile, the federal government counted 27 individuals in Oregon in 2024 whose ECT was billed to traditional Medicare. This federal dataset, though only a slice of the pie, facilitates regional comparisons—ECT appears to be far more widely used in the Midwest and Northeast than in the American West, for example. And it suggests fewer and fewer people have been receiving ECT nationwide. (Source: Centers for Medicare & Medicaid Services)
It appears to be particularly rare in Oregon. Here, few offer the treatment, and few people get it in turn. Ranked by individual providers per capita who billed Medicare for ECT in the past decade, Oregon placed 47th. Ranked by Medicare beneficiaries per capita who received ECT, it came in 49th.
Maine ranked first. In 2024, the latest year on record, Maine had an astounding nine times more providers per capita who billed Medicare for ECT than Oregon. And a Mainer on Medicare was nearly 12 times more likely to get the treatment than their Oregonian equivalent.
Medicare, of course, does not document all treatments. But adding Medicaid and private insurance claims to the mix still turns up just 136 people who received ECT in Oregon in 2024—just over 3 in 100,000.
Marina’s family, and the medical records they provided WW, describe a tumultuous run over the past year through the world of Portland-area geriatric care—lengthy stays between psychiatric wards, insinuations that Marina simply sought attention or drugs, a referral to an adult foster home where she’d go on to break her hip. It was only at Adventist Health, where she was treated for said hip injury, that at the urging of the family, clinicians looked into and settled on the catatonia diagnosis.
A heightened dose of the anxiety drug Ativan bolstered the theory that, within the shell remained a woman who could be retrieved. “I was there the first time she got it,” Nick recalled. “It was like she woke up from a dream, and was like, ‘Hi, Nick. Where am I? What’s going on?’”
The medication, thought to be unsuitable at this level in the long haul for someone of Marina’s age and condition, wore off, and she withdrew to her prior state. But the diagnosis seeded new hope. “The thought was, we know what it is, but it’s not going to last, treating her with this,” Benjamina tells WW. “The next step would be ECT.”
 Marina received her catatonia diagnosis at Adventist Hospital, where she was being treated for a broken hip after leaping from a bed. (Courtesy of Nick Brown)
Marina received her catatonia diagnosis at Adventist Hospital, where she was being treated for a broken hip after leaping from a bed. (Courtesy of Nick Brown)
The question was where. Kaiser’s Sunnyside Medical Center offers the treatment, but only to members. Legacy Health doesn’t offer it at all—though, reached for this story, a spokesperson said the system planned to in the future. Providence Health & Services has lacked a regular ECT program in Oregon since 2023; “there aren’t enough trained clinicians available,” a spokesperson said. Similarly, a provider departure is why St. Charles Health System in Bend says it discontinued its ECT program in spring 2026, just months after it launched.
Oregon Health & Science University is the big exception. It closed its inpatient psychiatric ward in 2017, coinciding with the opening of the Lloyd District’s Unity Center for Behavioral Health, but has continued to offer ECT as an outpatient service.
The first consultation with OHSU would have been virtual. But, after a referral from a Hawaii psychiatrist, the university’s ECT team initially refused to see Marina while she was admitted at another hospital, presenting the first Catch-22 of many. “She is not going to be stable enough to be in outpatient to get an evaluation to get ECT because she has catatonia,” Nick says. “And because she has catatonia, the real treatment she needs is ECT.”
As Marina grew weaker, the Browns, a family with means and uncommon medical expertise, found the Portland-area health system either unable or unwilling to coordinate within itself to accommodate Marina’s needs. Many hospitals seemed to want nothing to do with her at all. By January, however, they forged an arrangement: Marina transferred from Providence Milwaukie Hospital’s Psychiatric Unit to Unity, where she would stay during a run of outpatient ECT sessions at OHSU, scheduled to commence the following Monday, Feb. 2.
“We’re like, phew,’ Nick says. “‘Finally. Promised land. Right?”
 Marina returned in 2016 to Bolivia, where she and Bill met decades ago. Marina returned in 2016 to Bolivia, where she and Bill met decades ago. (Courtesy of Nick Brown)
Marina returned in 2016 to Bolivia, where she and Bill met decades ago. Marina returned in 2016 to Bolivia, where she and Bill met decades ago. (Courtesy of Nick Brown)
ECT is not new. It was in the 1930s that a Hungarian psychiatrist, applying the theory that people with epilepsy didn’t develop schizophrenia, decided to induce seizures in a psychiatric patient. The theory was wrong but, several chemically induced seizures later, the catatonic mute patient reportedly began to speak. Later, Italian researchers introduced electricity, and the crudest early forms of ECT were born.
Why it works remains a matter of debate; some think seizures disrupt a nerve pathway tied to major depression, prompting the brain to reinstitute a normal pathway. Whatever the case, the treatment, conducted on awake patients, was terrifying and ugly, involving thrashing, broken bones, torn ligaments, broken teeth.
The version everyone knows—even through cultural osmosis if you haven’t actually read or seen it—is tied to Ken Kesey’s novel One Flew Over the Cuckoo’s Nest and Jack Nicholson, who in the 1975 film shot at Oregon State Hospital, shakes madly under the electrodes’ barbaric power.
The film shaped public perception for generations, contributing to the deinstitutionalization movement that refashioned Oregon’s mental health system in ways that linger to this day—and to a particular, well-documented aversion to ECT among the public and medical profession alike. Decades later, the treatment remains to some about as reputable as a lobotomy.
Anesthesia, muscle relaxants, and paralyzing medications render the modern version of ECT a “safe, benign, boring looking procedure,” says Dr. Anna Borisovskaya, a psychiatrist in Seattle.
Yet the film cast a long shadow, and other sordid associations have not helped. The Church of Scientology, a sworn enemy of the psychiatric profession, has fixated on ECT to the point that some practitioners, wary of attracting attention, avoid speaking publicly about their work to this day. Others, when they hear ECT, may recall its use as a “cure” for homosexuality, or the MKUltra affair, when the CIA deployed electroshock, LSD, and other techniques to the cause of mind control.
More mundane forces shaped ECT’s development too. Regulators viewed it with suspicion. The psychiatric profession turned hard to pharmaceuticals. ECT reimbursed poorly—while requiring expensive hospital space and personnel, including not just an ECT provider who could probably make more money delivering outpatient care, but nurses and an anesthesiologist, who may be wary of the procedure themselves.
Even many psychiatrists know little of the treatment. Several tell WW of getting scant exposure to ECT in medical school or residency; those who took it up had to go out of their way to do special fellowships, where practitioners like Matout of Stanford say they witnessed remarkable results firsthand. “Once you become more exposed to it,” he says, “the stigma is reduced.”
Marina never got the ECT. At Unity, Nick says, she tripped on her long scrub pants, hit her head and, by the end of January, was in OHSU’s Intensive Care Unit. Subsequent imaging showed a subdural hematoma—an internal brain bleed, which posed new risks for ECT. Marina was, the OHSU team informed Bill when the doctors did their rounds, no longer a candidate for the treatment.
In the first of many interviews for this story, Nick emphasized that he and his sister Benjamina get along well in the medical community, the point being that they aren’t some embittered quacks, eager to cast aspersions. And yet, he has found his family’s experience with OHSU—where he and his sister were themselves trained—to be disturbing, a sign of a system incapable of taking feedback or seeing a patient in the context of their whole life.
It is the position of the American Psychiatric Association that there is no absolute contraindication for ECT. Considerable literature exists on the risks brain bleeds pose, and circumstances in which ECT is nonetheless advisable. Nick found this literature. And the questions that emerged were clear. If Marina didn’t get ECT, there was reason to believe she would be catatonic for the rest of her life. So why not do the treatment, despite the risk? Or at least discuss it?
The Brown family says the chief ECT provider at OHSU, Dr. Anne Fang, and the team she oversaw, had little interest in such a discussion. The family pressed their case. “They fear that we have given up on her, and that she will ‘just go home to die,’” a doctor wrote in a Feb. 13 patient note, adding that the “family unanimously believes she would rather die than to live in this condition, even if the treatment (ECT they very much want) is what ends her life.”
Despite these entreaties, Nick and others in the Brown family say the hospital had declined to brook a serious conversation about the ethical tensions at play—or even, for that matter, facilitate a second opinion in say, Seattle, where more ECT providers work.
In the note, the OHSU doctor wrote that it would be difficult “logistically as well as ethically” to “attempt to convince another place to provide a treatment that we have deemed is inappropriate.”
Nick saw this as a terrible argument; he says he never pushed the OHSU team to “convince” another institution to provide ECT, but merely to seek further counsel for a complex case he suspected was out of their comfort zone. In any event, the conversation stalled. Overriding the family’s appeal, OHSU, offering a third-line medication treatment for catatonia, discharged Marina on Feb. 23.
When, a few days later, WW encountered Marina at her and Bill’s home on that foggy morning in Sellwood, she barely said a word—and what sounds she made emerged as near-unintelligible whispers. What movements she made appeared confused and tentative, but she had an outpatient neurology appointment at OHSU to get to. Bill, Nick, and a young nurse they had hastily arranged to hire ushered her gingerly to the car.
“Careful, Marina,” Bill said, and she shuffled toward the open back-seat door. Entering, she bumped her head on the door. For a moment, the world stopped. Was she OK? She seemed OK. Bill drove across the river and up the hill to OHSU for imaging. Later that morning, the neurosurgeon reported that the hematoma was healing up. A few weeks later, doctor notes show, he said the hematoma had resolved—and “expressed agreement” with pursuing ECT.
 Diagnosed with catatonia in late 2025, Marina has been home from the hospital since February. Her family fears she will die without ECT. (JP Bogan)
Diagnosed with catatonia in late 2025, Marina has been home from the hospital since February. Her family fears she will die without ECT. (JP Bogan)
Borisovskaya, the Seattle psychiatrist, heard little of ECT in medical school, but in time became a true believer. Her turning point came around 2010, when she became an attending physician at the city’s VA Hospital, a place of great need, she says, yet where ECT was treated as a burden and an annoyance.
But Borisovskaya was faced with a psychotic patient who had intended to kill himself and his family. She dove into the ECT literature, got certified, and performed the treatment on the patient herself. “He went,” she says, “from being like a zombie to looking just like one of the happiest people I have ever met.”
She realized that ECT was “the most important thing that I can do with my life right now.” She ramped up the ECT program at the Seattle VA, taking referrals from far and wide. In 2021, she moved on to a private clinic, SeattleNTC.
It was here, on March 4, that she met Marina. Nick had connected with SeattleNTC via one of the psychiatrists across the nation from whom he’d sought counsel, and that morning the Brown siblings—two flanking Marina in the back seat to ensure she didn’t bolt from the moving car—escorted her north to the evaluation.
Borisovskaya did not find Marina’s case (which the family gave consent for her to discuss) to be straightforward. The catatonia diagnosis seemed reasonable, but the presentation was atypical: Marina, she says, seemed uncommonly agitated for a catatonic person, and despite dementia having been ruled out, it may have crept in subsequently. Meanwhile, Marina’s history of brain injury could indeed pose a “significant” risk of brain bleeding—a potential killer.
And yet, Borisovskaya says, ECT does tend to work for atypical cases. She felt Nick understood the dangers well, and she sympathizes deeply with the family’s predicament. She believes Marina may not be a “good” candidate for ECT, but that she is still a “reasonable” one. And she believes no other good options remain.
Though the family said it would consent to a discussion of Marina’s case with WW, OHSU declined the offer. “In general, ECT is a safe and effective treatment for catatonia,” spokesman Erik Robinson said. “Still, we have to consider all of the complexities of any patient’s past medical and psychiatric history, and anticipate potential complications and safety concerns.”
He added that OHSU convenes multidisciplinary conferences to help balance risks and benefits for complex cases, and that “even though we can’t always deliver the treatment they request, Oregonians should know that OHSU carefully considers the unique circumstances of each patient—and our heart goes out to every family in these hard positions.”
Given the nature of this story, OHSU declined to make its experts available to discuss ECT, but referred WW to a provider in Eugene. Dr. Nicholas Telew has been practicing ECT in Oregon since 1991, and recalls long periods in which access to treatment in the state was scarce.
He believes ECT saves lives—and particularly those of elderly people with catatonia. Such patients, he says, tend to “dwindle and die.” Often they were diagnosed with dementia and sent off to a memory care home. “Occasionally, someone at the nursing home says, ‘I don’t think this is really true dementia,’” he says. “And they get referred to me and I treat them and they’re back to normal for the rest of their life.”
At this point in the conversation, Telew knew little of Marina’s case. Told of it, his voice rose in disbelief. Teaching hospitals like OHSU, he said, are supposed to take the hard cases. “That’s so unconscionable,” he said. Told that the hospital believed the case was too risky, he responded, “Well, yeah, of course you advise the family of the risk and benefits and say, ‘There is a possibility she could have a bleed.’”
OHSU did not respond directly to Telew’s criticism. Telew says he’d be open to taking a look at Marina. Meanwhile, alternatives dwindle. In recent weeks, the Browns were arranging with a lawyer to transfer Bill’s guardianship to Washington state, as Borisovskaya advocated for a hospital in Seattle to let her give Marina ECT herself.
A few days ago, Borisovskaya informed Nick this path had stalled: The health system legal team did not believe the Washington guardianship requirements had been met. “Basically, a refusal,” Borisovskaya wrote. “I’m genuinely disappointed and concerned on your behalf. I would have loved to do ECT for Marina…I wish things were different.”
One afternoon a few days later, Bill sat beside Marina on a couch in their Sellwood home, reflecting on the outcome. He’s been bewildered, he says, by the way health care institutions don’t seem to talk to each other, coordinate with each other.
Marina’s eyes fluttered and she shook her head, seeming agitated. Bill tried to coach her to calm down, and she did. He glanced over at Marina. “She still has the best smiles,” he said.
Marina had said little to this point but seemed to be perking up. Asked how she was doing, she whispered that it was not a good day. “It’s strange,” she said, adding that she did not know if this was really her home. Eventually, she got up, trailed by a home health aide seeking to keep her from falling, and shuffled around in her blue socks, looking at old photo albums of friends from their travels, and from her wedding six decades ago. Asked about her favorite art, she made her way to a massive Buddha head sculpture. “I love my Buddha head,” she whispered, rubbing it.
The aide took Marina to rest, and Bill went outside to his porch and reflected on Marina’s daily rhythms. “Every day starts with a smile,” he said, but then she recedes, starts to shake, and loses contact. Medications sometimes have fleeting effects, and sometimes, in the early afternoon, she shows flashes of the old self. A few times, he said, he’s put on a song—Johnny Cash, say—and she seemed to respond well.
“She loved to dance,” he said. “She loved it before. She loves it now.”
 Bill (pictured) and Marina Brown bought this house in Sellwood more than a decade ago, before her decline. (JP Bogan)
Bill (pictured) and Marina Brown bought this house in Sellwood more than a decade ago, before her decline. (JP Bogan)