
Overview
People receiving treatment for substance use disorders (SUDs) have a range of health and life goals. Their work toward these goals is often referred to as recovery, which the federal Substance Abuse and Mental Health Services Administration (SAMHSA) defines as “a process of change through which individuals improve their health and wellness, live self-directed lives, and strive to reach their full potential.”1 Recovery is not a one-size-fits-all outcome, and it doesn’t always mean abstinence from substance use.2 For many, recovery is about building a better quality of life—and that can include finding stable housing, securing employment, being freed from incarceration, rebuilding relationships, and regaining custody of children.3
Measuring recovery allows jurisdictions—in this case, U.S. states, territories, and the District of Columbia—to assess whether services provided by SUD treatment settings and recovery-related organizations help people move toward their goals. It can also help jurisdictions to identify and address areas for improvement in recovery-related services. Such metrics can be beneficial, as studies have shown that recovery services can deliver substantial returns on investment.4 For example, a recovery housing program—a supportive environment that provides stable housing for people in recovery— located in Florida generated a net benefit of $143 million over 20 years, with a return of $22.19 for every dollar invested.5
In the SUD cascade of care, a framework that measures service effectiveness throughout treatment, recovery is the final stage. In 2021, The Pew Charitable Trusts convened an expert panel to select a set of core opioid use disorder (OUD) treatment measures along the cascade of care that could help states to assess their OUD treatment systems and identify areas for improvement. As a result of this effort, Pew recommended that states work with people with lived expertise—deep knowledge and insights gained over time through their experience navigating systems for themselves and others—to test existing recovery assessment tools and select measures for appropriate outcomes. Because no nationally endorsed standardized recovery measures exist, the expert panel did not endorse a specific measure or recovery measurement tool.
However, established instruments for assessing recovery and recovery capital (i.e., recovery support resources such as assistance with obtaining employment) are available.6 The instruments vary, but they generally consist of a series of questions about an individual’s life, such as employment or housing status, sense of well-being, connection to family and community, and resources available through networks.
Recovery measurement efforts take place at the recovery organization and treatment settings and at population levels (e.g., a population-wide survey distributed by the state). Jurisdictions can require treatment providers and recovery community organizations to assess the recovery progress of the individuals they serve. At the population level, a broader approach can address community health and well-being. Data collected at the setting and population levels can help jurisdictions and service settings with client recovery planning, quality improvement, and shaping of policies and programs. These efforts could also equip clients with tools to track their progress toward their recovery goals.
To understand how jurisdictions are implementing recovery measurement efforts and what tools they are using, Pew surveyed behavioral health officials in all 50 states, D.C., and U.S. territories. The questions focused on whether jurisdictions have engaged in initiatives using setting-specific efforts or a population health approach, and on the scope of the initiatives, the measurement tools used, and barriers and challenges associated with measuring recovery. Officials representing 39 jurisdictions responded to at least one question.
Based on findings from this survey, Pew recommends:
Measuring recovery and/or recovery capital in key treatment and recovery service settings or jurisdiction-wide.
Agencies such as a state department of behavioral health can direct service settings to use established, feasible recovery or recovery capital measurement tools such as the Brief Assessment of Recovery Capital Scale (BARC-10) or the Addiction Severity Index.
Involving people with lived expertise in recovery measurement efforts.
Jurisdiction agencies should engage people in recovery—along with youth and family members—in all stages of measurement initiatives, including selection of recovery measurement tools and interpretation of data.
Disaggregating recovery data by demographic variables.
Jurisdiction agencies should analyze recovery measurement outcomes by race, ethnicity, gender, socioeconomic status, and other demographic factors to uncover differences among populations and inform targeted interventions.
Streamlining federal data collection requirements.
SAMHSA should continue to revise data collection requirements to allow for recovery measurement initiatives.
Defining and supporting recovery
People with personal experience of substance use define recovery in various ways, so recovery cannot be measured by any one indicator.
But research has found commonalities in what people with SUDs want out of their treatment and recovery. One nationwide survey of nearly 900 people with a SUD found that the number one priority was simply staying alive. The second most reported priority was improved quality of life; stopping of all drug or alcohol use came third and was not reported by all respondents.7 Not everyone who uses drugs or engages in treatment finds meaning in the term “being in recovery”; some even reject that label.8 Yet that does not mean they do not also wish to stay alive and improve their quality of life.9
Recovery capital is defined as “the breadth and depth of internal and external resources that can be drawn upon to initiate and sustain recovery.”10 There are several types of recovery capital, including social (e.g., family), physical (e.g., safe housing), cultural (e.g., culturally responsive care), community (e.g., behavioral health facilities and other settings further described below), and human (e.g., specific knowledge) capital.11
Regardless of terminology, when people engaging in recovery services set individual goals and receive support in achieving them, their quality of life can improve.12 This support can also yield important economic benefits in the form of reduced health care costs and increased employment.13 People with SUDs can achieve their goals with a variety of services and supports, including but not limited to:
Peer recovery workers: Peers are people with lived and living experience of SUD who work in a variety of behavioral health settings, such as treatment centers, hospital emergency departments, recovery-focused organizations, and mobile outreach vans that provide naloxone and drug-checking equipment.14 Peers play a vital role across settings—including nontraditional health care settings such as the criminal legal system—by enhancing treatment engagement, providing emotional and educational support, and increasing connections to care.15 In addition, research has found that peer recovery coaching can lead to health-related cost savings and potentially lower health care system expenditures through enhanced outcomes and reduced reliance on acute care services.16
Recovery community organizations (RCOs): These nonprofit organizations are led by people in recovery.17 They provide peer recovery support services, organize recovery-focused education and outreach, and advocate for policies that support recovery.18 RCOs also host community events, offer training to build the recovery workforce, and support the development of recovery institutions such as recovery cafes, reentry programs, and employment services.
Recovery housing: These supportive environments, also known as recovery residences, promote recovery through peer support and structured living.19 Research shows that recovery housing is associated with improved outcomes in abstinence, employment, and income and is more cost-effective than standard continuing care or other residential interventions.20 Recovery homes vary in intensity and services, from peer-run homes to clinically staffed residences. The National Alliance for Recovery Residences (NARR) defines several levels of recovery homes based on structure, staffing, and services provided.
Treatment settings: SUD treatment is delivered across a range of settings tailored to individual needs. For example, federally certified opioid treatment programs (OTPs)—the only facilities that can legally dispense methadone—can also provide other medications for OUD.21 Providers in office-based opioid treatment prescribe medications including buprenorphine and naltrexone in outpatient settings, expanding access to care.22 Other settings include residential programs for 24-hour care, intensive outpatient programs for frequent treatment without overnight stays, and standard outpatient care for people needing less intensive support.23
Other health care settings: Hospitals, primary care clinics, emergency departments, behavioral health centers, and stabilization centers—which are crisis support facilities that offer SUD assessment, care, and referrals, though not exclusively—are critical access points for identifying and treating SUDs. These settings can provide screening, initiate medications for treatment, manage co-occurring conditions such as mental and physical health problems, and refer patients to specialized services.24
People in or seeking recovery can also benefit from less formal supports such as mutual help groups like Alcoholics Anonymous or SMART recovery peer support groups that meet independently of recovery or treatment organizations. Because these groups are autonomous and don’t receive public funding, they were not included in this research project.
Additionally, other community-based organizations serving people who use drugs provide critical life-saving services, such as sterile syringes, naloxone, and drug-checking equipment; some also offer buprenorphine for people with OUD. These organizations are often led and staffed by peers and play a vital role in improving quality of life and increasing the number of people receiving treatment.25 While these settings were not explored in this research project because the focus was on recovery community organizations and more traditional treatment settings, approaches that help to reduce harms associated with drug use can support multiple pathways to wellness and align with the individualized goals of people in recovery.
The importance of measuring recovery
To understand whether treatment and recovery services are effective, jurisdictions and service settings should conduct recovery assessments. Systematically tracking recovery outcomes also helps organizations to demonstrate the value of recovery supports (for example, using peer recovery workers), secure funding, and guide continual quality improvement.26 Tracking ensures that services are aligned with the goals and needs of people in recovery. Because recovery is a dynamic and individualized process, measuring it requires tools that reflect different pathways and definitions of success.27 These measurement tools exist, and jurisdictions have used a variety of them to measure recovery at the population or service setting level. Recovery measurement not only supports accountability for recovery service organizations but also empowers peer workers and people in recovery by validating their progress and experiences.28
Advancing Value-Based Payment in SUD Care Through Recovery Measurement
Integration of recovery measurement into value-based care models presents a powerful opportunity to transform the broader SUD treatment system.29 Unlike traditional fee-for-service models, value-based approaches can reward providers for delivering coordinated, person-centered care that can support sustained recovery. However, widespread adoption of value-based approaches faces challenges, including limited infrastructure, insufficient quality measures, and lack of provider readiness.30 Jurisdiction agencies can address these barriers by developing patient-centered outcome metrics or in this case using established recovery measurement tools, providing technical assistance to organizations, and expanding provider capacity.31
By integrating recovery measurement into value-based payment models, systems can better capture the full impact of recovery support services on real-life outcomes such as reducing emergency department visits or retaining employment. This approach could help more people get the care they deserve while making the system more effective and affordable.32
The first step in transforming the SUD treatment system into a value-based care model is establishing the feasibility of widespread recovery measurement.
Survey results show progress toward measuring recovery
Recovery assessments are required in certain service settings; some jurisdictions measure recovery population-wide. Pew’s survey found that recovery measurement is feasible, as demonstrated by the number of responding jurisdictions that have implemented these efforts.
Of the 38 state behavioral health agency officials who responded to the question asking whether they require certain settings to conduct recovery assessments, 18 stated that their jurisdiction has these requirements while 13 indicated that their state did not. Seven officials did not know whether their jurisdiction requires settings to assess recovery.
Twelve jurisdictions attempted to measure recovery from SUD at the population level, while the remaining jurisdictions that responded to this question did not attempt to measure recovery population-wide (23) or did not know whether this type of initiative occurred (3).
Jurisdictions most commonly required recovery community organizations to implement recovery assessments
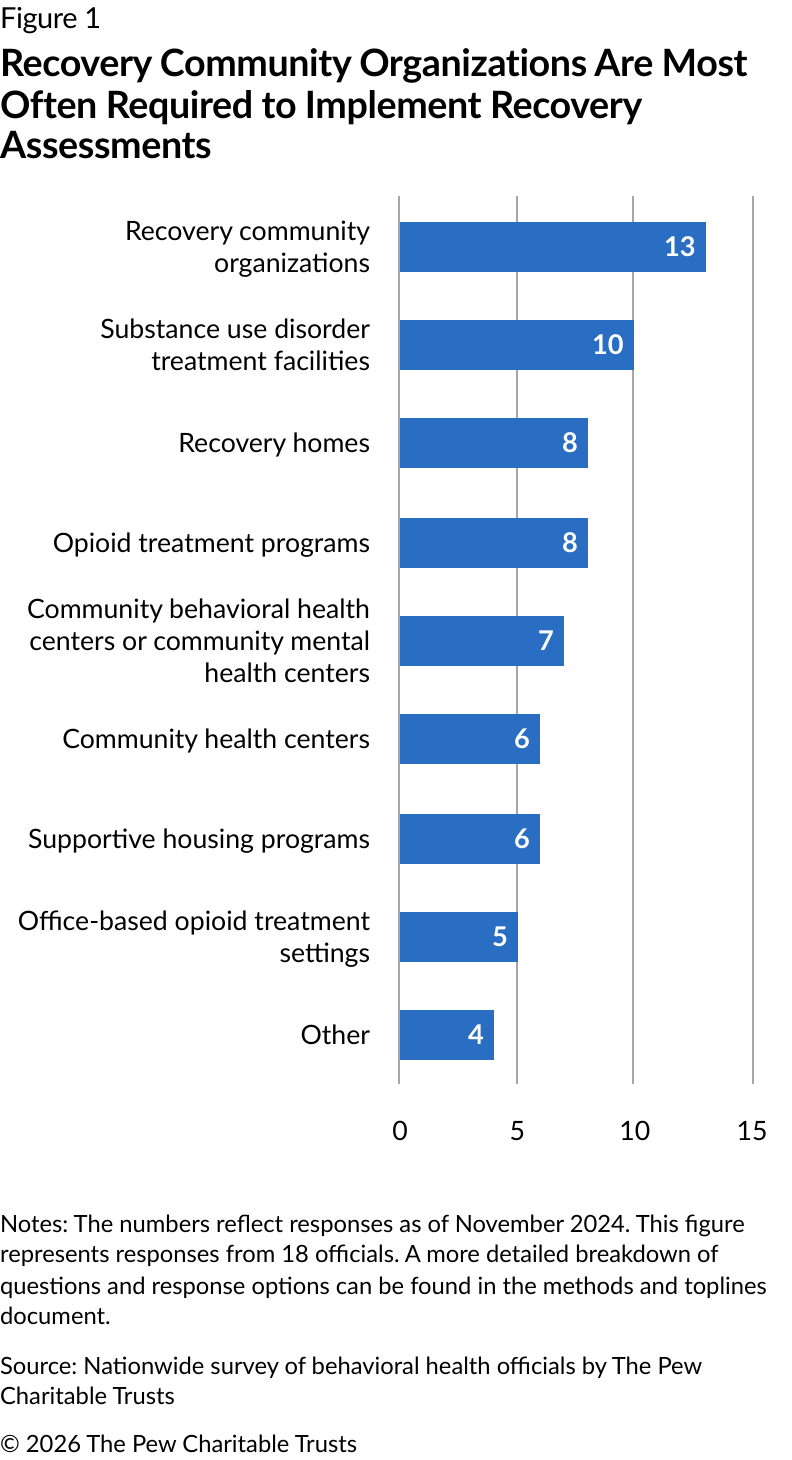
When Pew asked officials which settings were required to conduct recovery assessments, of the 18 jurisdictions that required settings to do so (Figure 1):
Thirteen officials said their state requires recovery community organizations to implement recovery assessments.
Ten officials indicated that their state required SUD treatment facilities (other than settings specializing in medications for OUD) to conduct these assessments.
Eight jurisdictions required recovery homes and OTPs to implement them.
Quality improvement initiatives often require settings to conduct recovery assessments
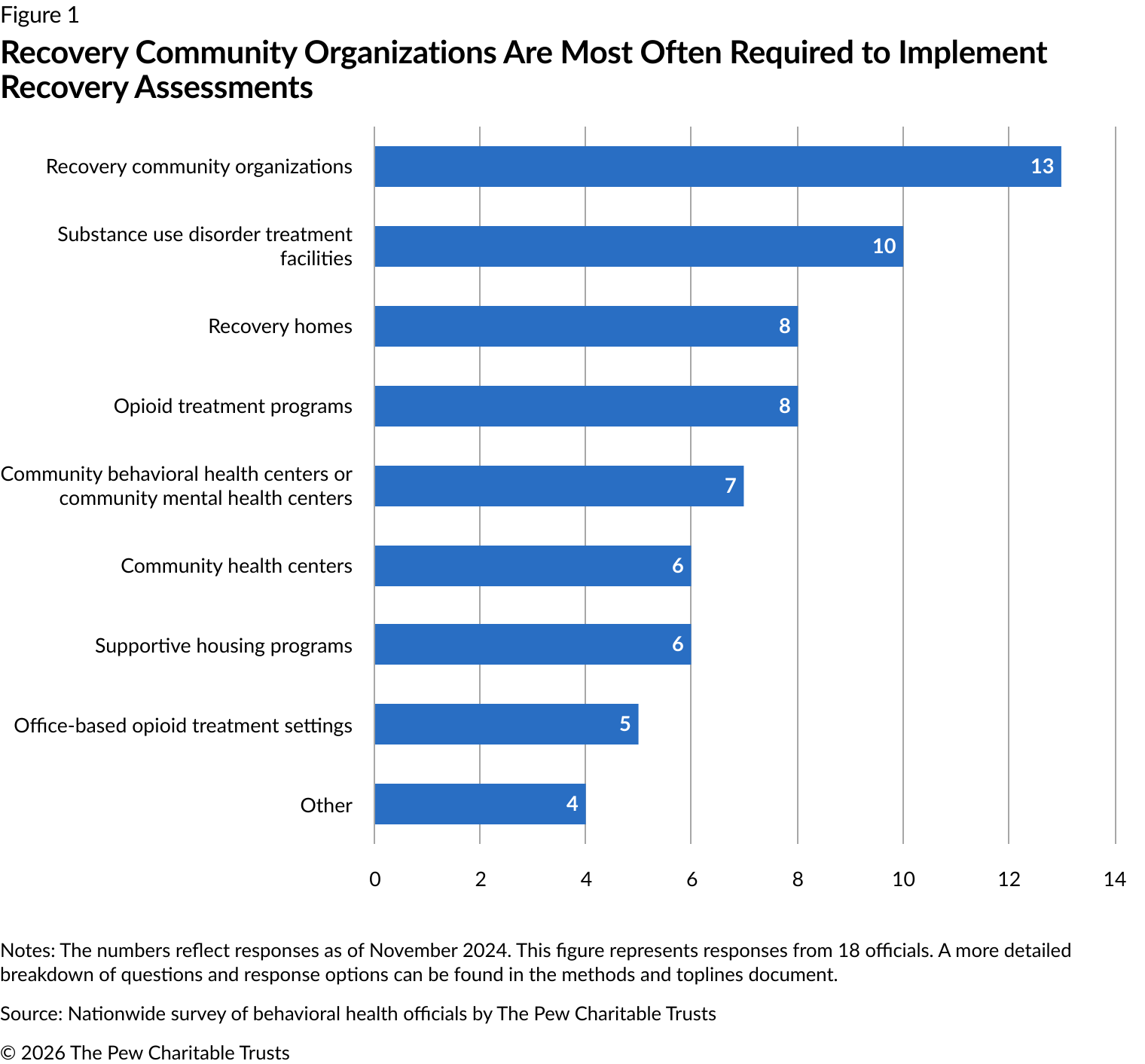
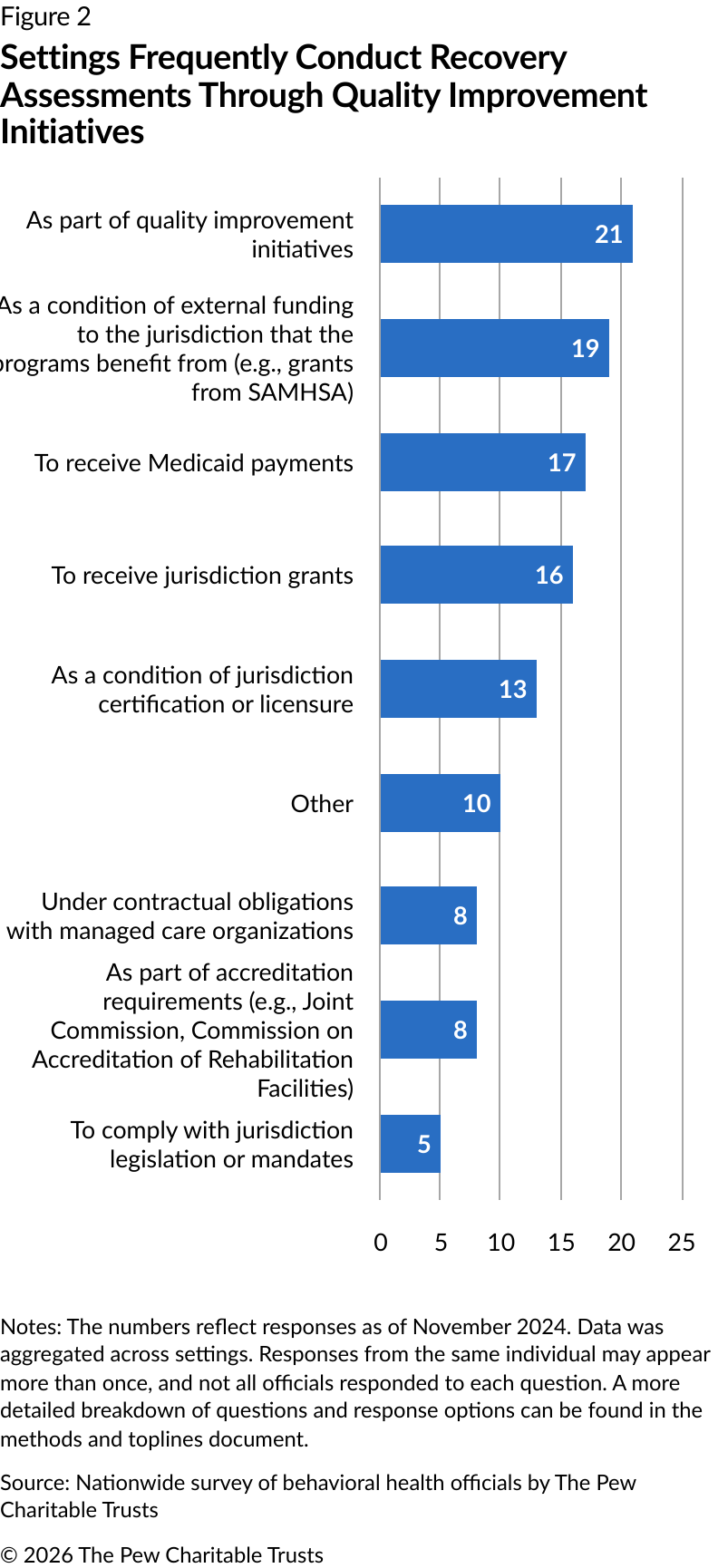
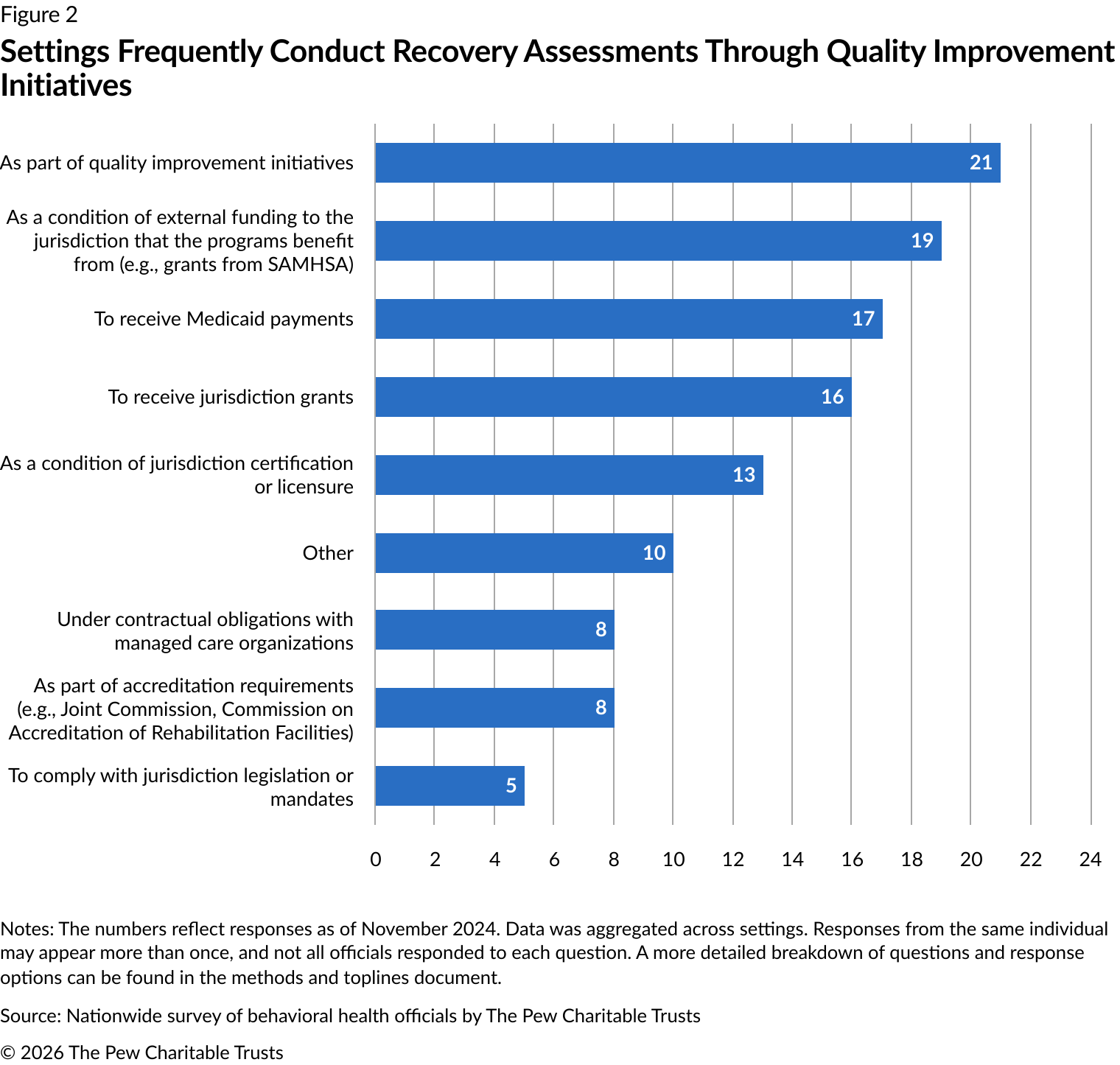
Officials identified myriad reasons for requirements that settings conduct recovery assessments (Figure 2). Quality improvement initiatives were the leading reason, as identified in 21 responses. This was followed by external funding requirements such as federal grants (19 responses), Medicaid payment requirements (17 responses), jurisdiction grant requirements (16 responses), and conditions of licensure (13 responses). Although requirements varied by setting, RCOs were most frequently required to conduct recovery assessments to receive external funding (eight responses) or jurisdiction grants (six responses).
Some recovery assessment instruments are used more often than others
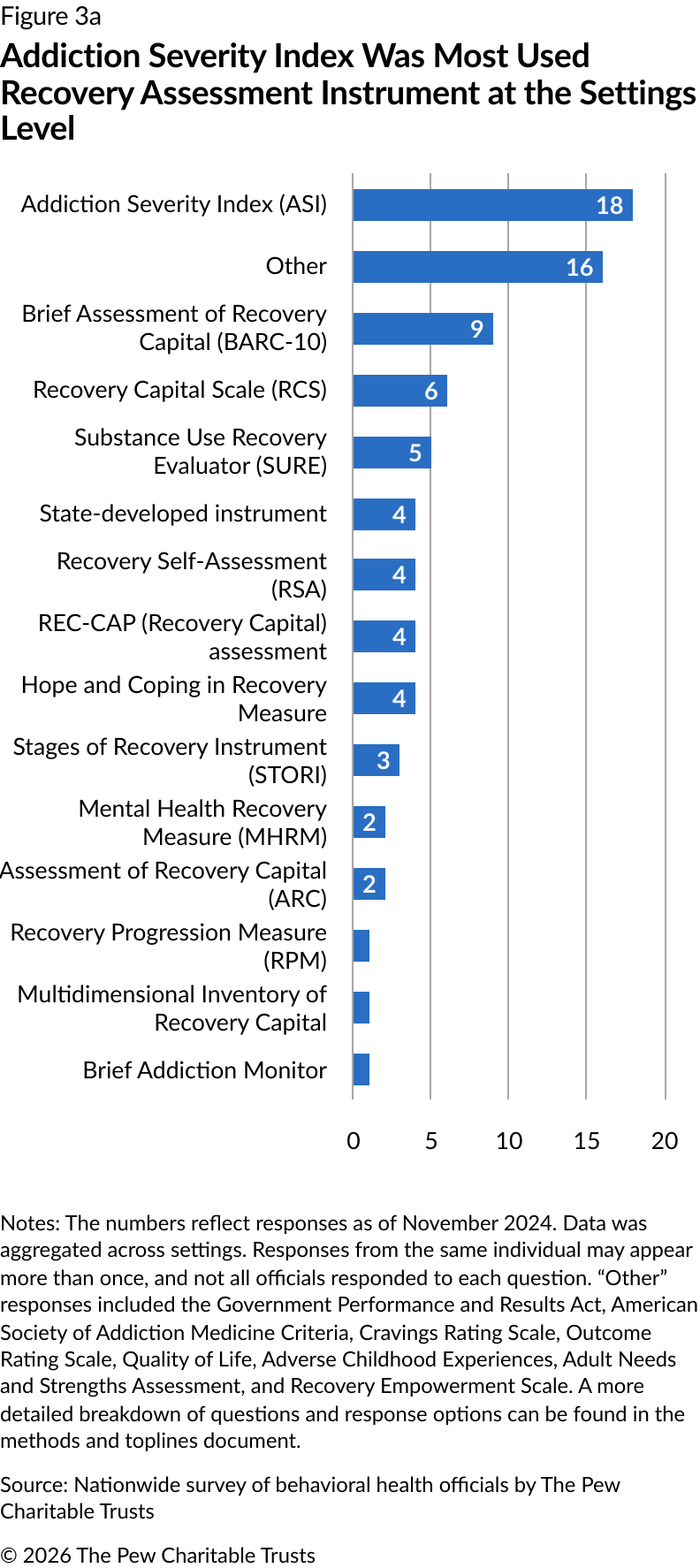
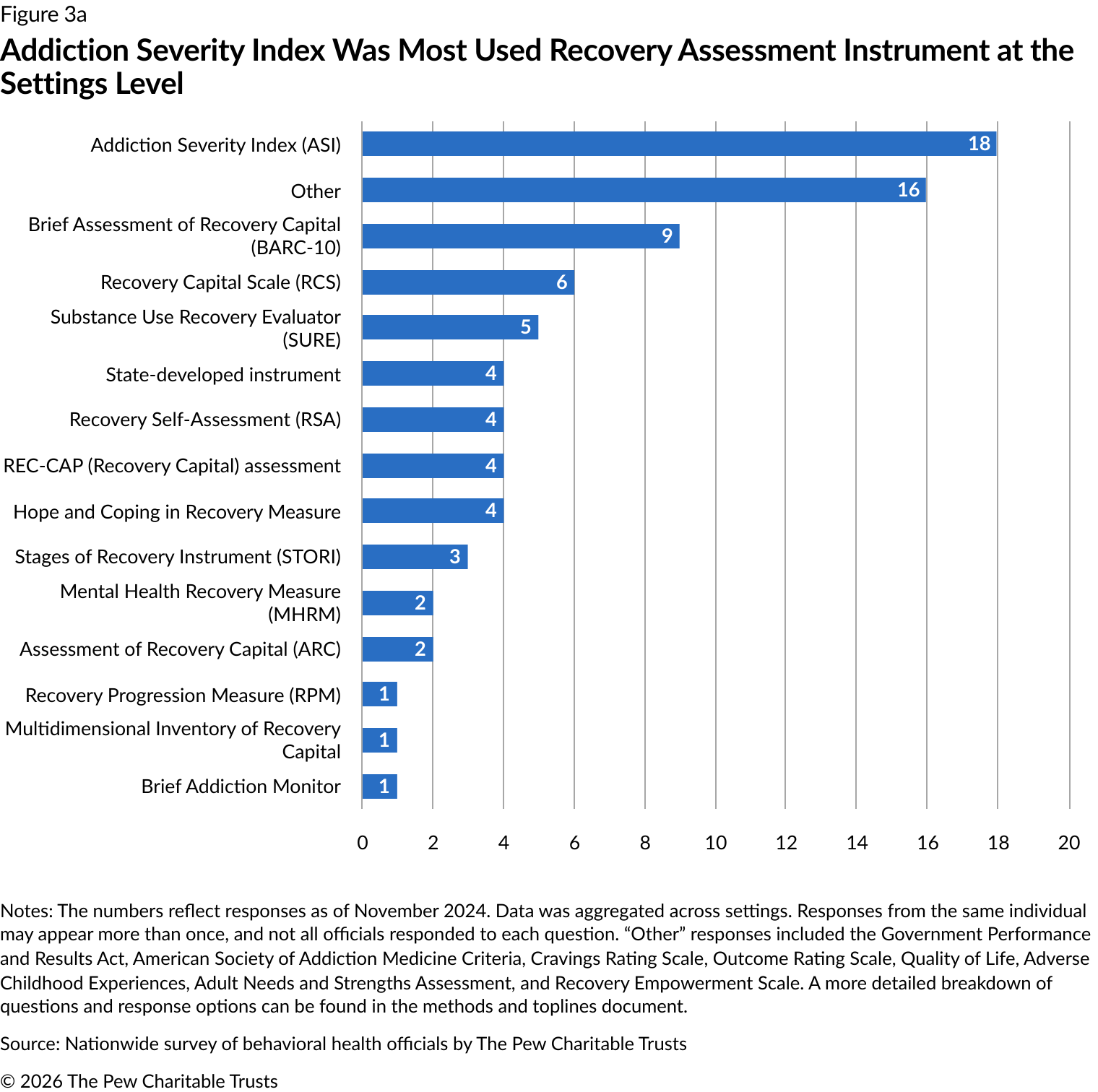
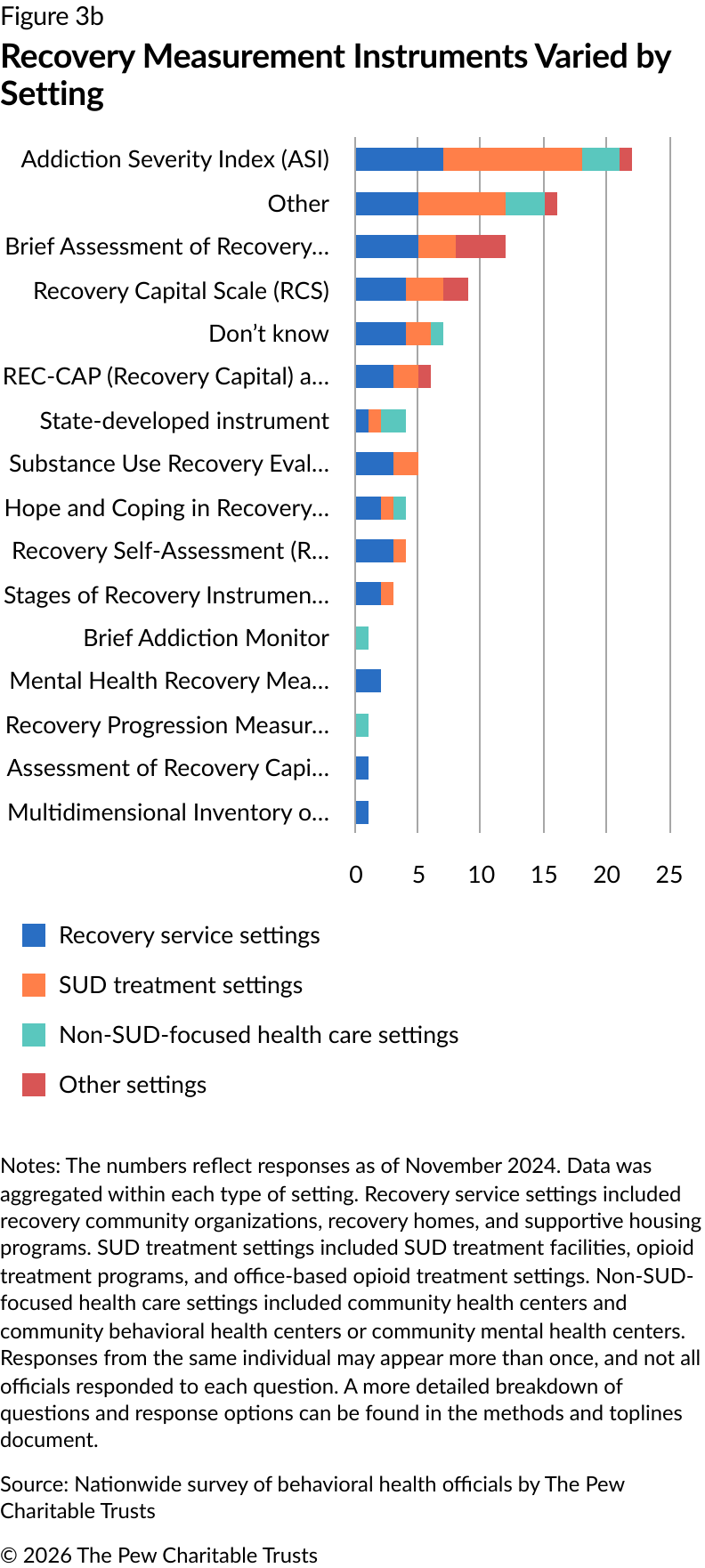
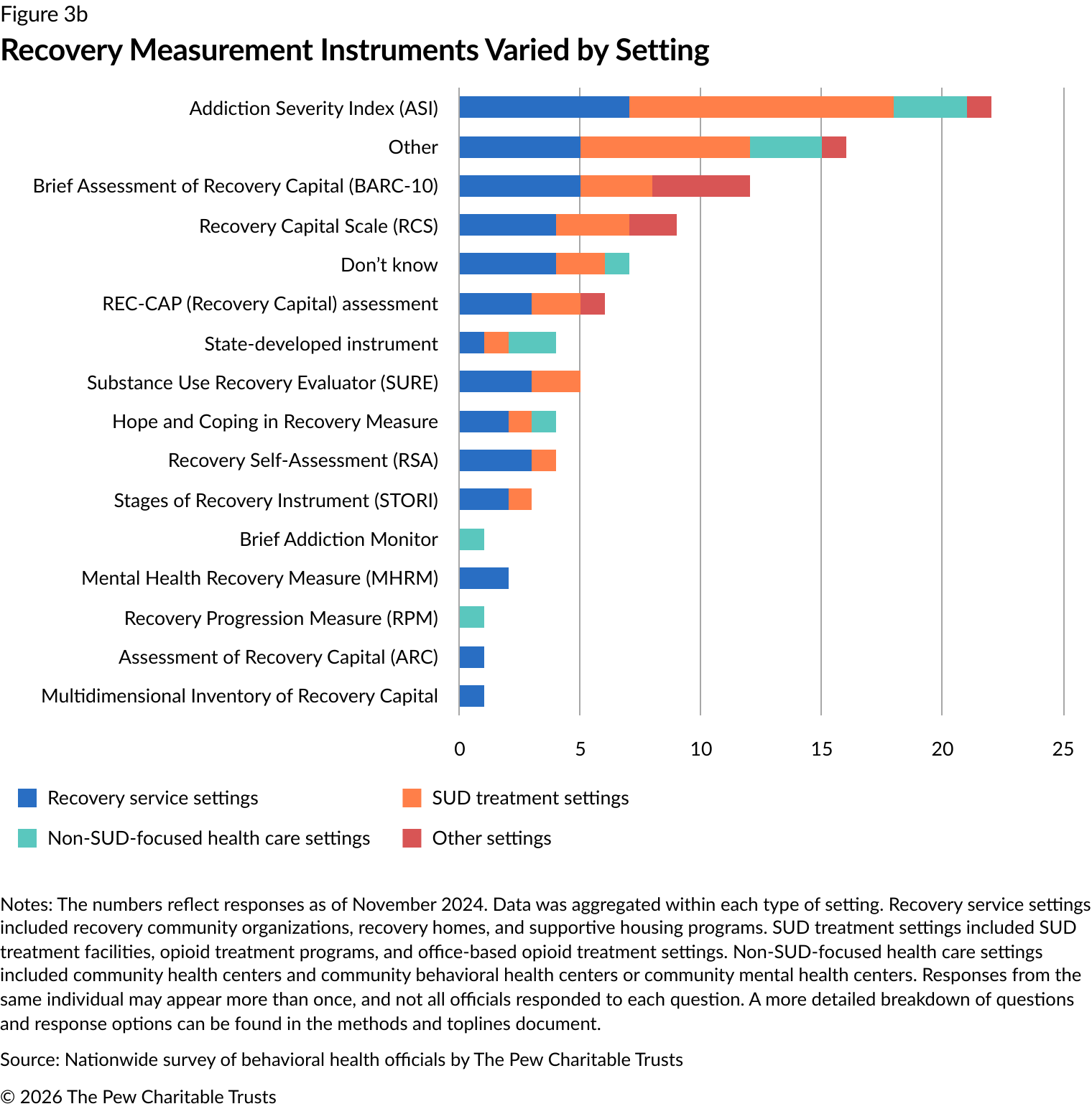
At the settings level, the Addiction Severity Index (ASI) was the most used recovery assessment instrument (18 instances). The Brief Assessment of Recovery Capital (BARC-10) was the next most common, reported nine times. The Recovery Capital Scale (RCS) and the Substance Use Recovery Evaluator (SURE) were reported six and five times, respectively (Figure 3a). The recovery measurement tools that were used varied between settings. For example,
substance use treatment settings most commonly used the ASI, while recovery service settings used the BARC-10 (Figure 3b).
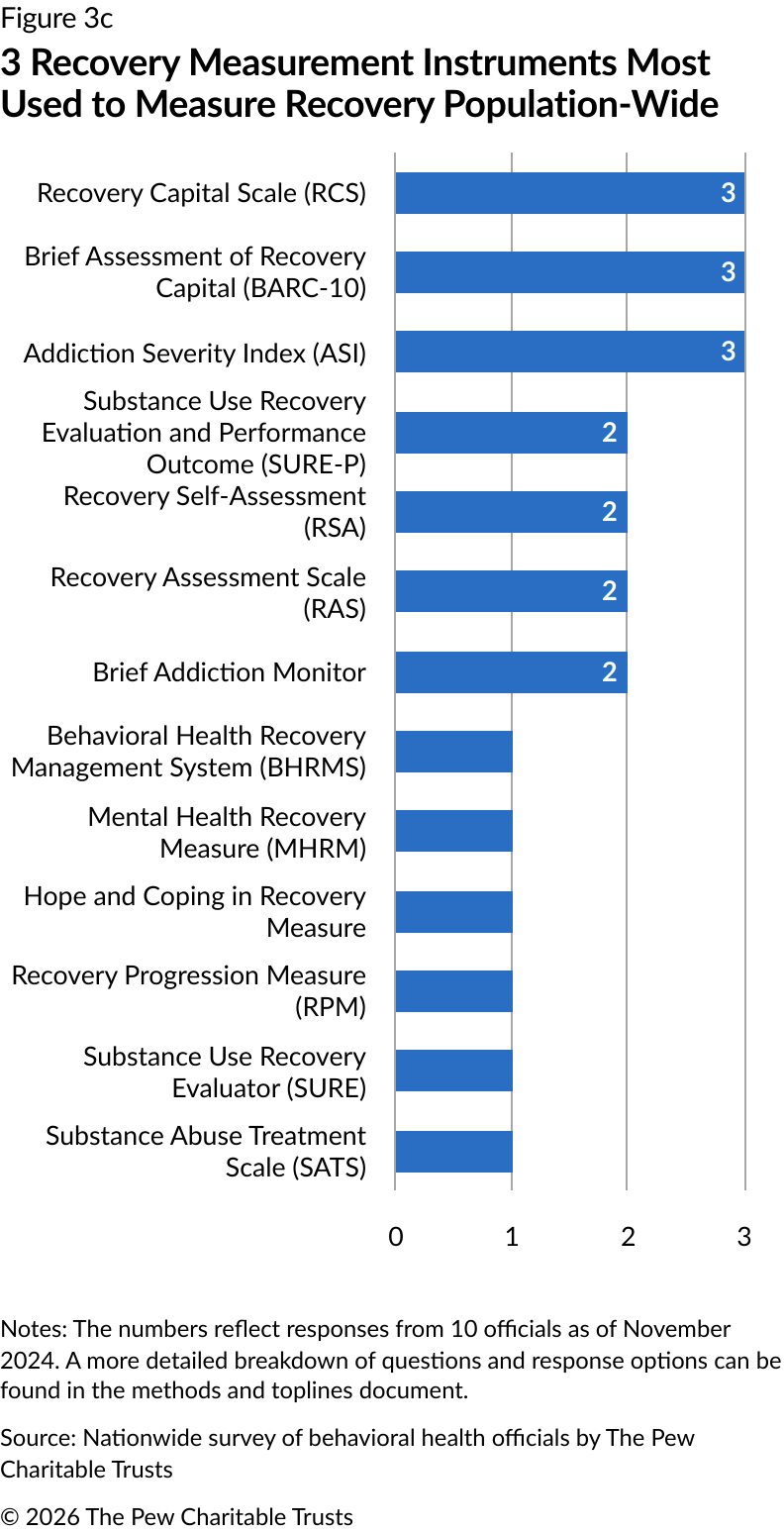
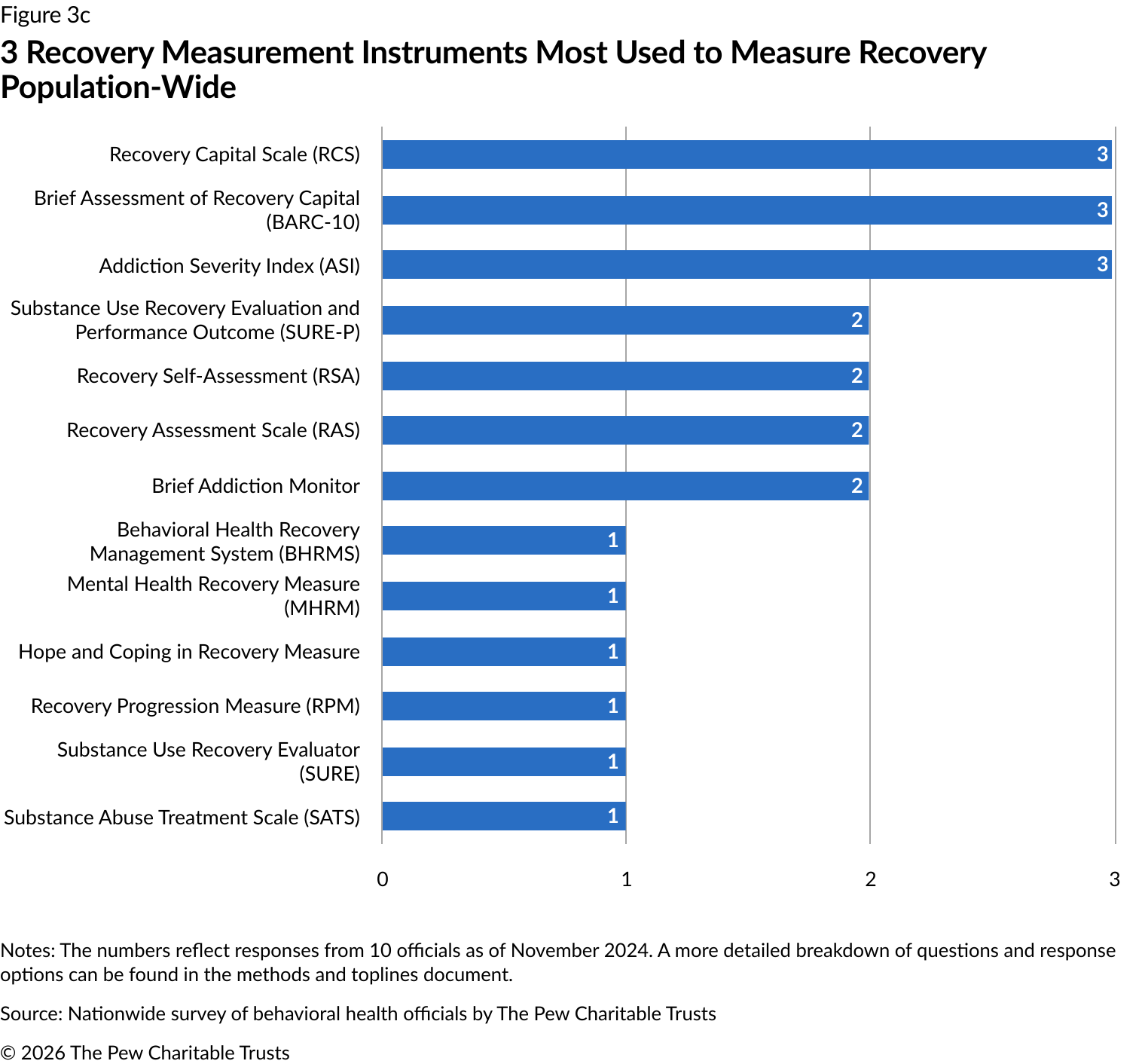
The ASI, BARC-10, and RCS were most commonly used at the population level, with each reported by three jurisdictions (Figure 3c).
Commonly used recovery measurement instruments
Settings can use a variety of tools to measure recovery, and although they often include questions about abstinence, substance use is just one of many areas assessed. These tools can also differ in other important ways. For example, the number of questions they include—ranging from brief screeners to more comprehensive assessments—and the way in which they are administered can vary from self-report surveys to structured interviews. These differences mean that tools also vary in complexity and time commitment. As a result, there is often a trade-off between the level of detail a tool provides and the amount of effort it requires from both providers and participants.
Pew asked officials to select which of 23 tools—identified through the Repository of Useful Scales, researchers, and experts from the recovery community—their jurisdiction used and/or whether any other assessment tools were used. Of these tools, four emerged as the most common:
Addiction Severity Index (ASI)
Designed as an approximately one-hour semi-structured interview in which participants are assessed across seven domains: alcohol use, drug use, medical, psychiatric health, employment/self-support, family relations, and illegal activity. Participants are assessed over the past 30 days as well as their lifetime. A six-month time frame is included for certain questions.
165*
Brief Assessment of Recovery Capital (BARC-10)
Self-report questionnaire derived from the 50-item Assessment of Recovery Capital (ARC). Items capture agreement with statements about recovery capital, which are various psychological, physical, social, and environmental factors that aid in recovery. This tool includes the following domains: substance use and sobriety, global psychological health, global physical health, civic and community engagement, social support, meaningful activities, housing status, risk-taking behavior, professional support, and recovery experience.
10
Created as a self-assessment tool to measure one’s degree of recovery capital. Participants rate their agreement with 35 statements on a scale of 1 to 5. After completing these questions, participants are asked to complete a Recovery Capital Plan that sets out goals to increase recovery capital.
35
Substance Use Recovery Evaluator (SURE)
Self-report tool designed with input from people in recovery. Includes 21 graded questions—scored or rated based on the participant’s responses—and five additional ungraded questions that are designed to promote participant reflection. Developed for private, therapeutic, or service outcome assessment or for research but not designed for residential settings. This tool includes the following domains: drinking and drug use, self-care, relationships, material resources, outlook on life, and recovery importance.
26
Note: Pew did not ask officials to specify which edition of the ASI was used in their jurisdiction.
*The number of questions included in the ASI varies depending on whether it is the initial screening or a follow-up, and not all questions are asked directly to the patient.
Sources: A. Thomas McLellan et al., “The Addiction Severity Index at 25: Origins, Contributions and Transitions.” John S. Cacciola, “Recent Status Scores for Version 6 of the Addiction Severity Index (ASI-6).” A. Thomas McLellan et al., “The Fifth Edition of the Addiction Severity Index.” Corrie L. Vilsaint, “Development and Validation of a Brief Assessment of Recovery Capital (BARC-10) for Alcohol and Drug Use Disorder.” “Recovery Capital Scale.” Joanne Neale et al., “Development and Validation of ‘SURE’: A Patient Reported Outcome Measure (PROM) for Recovery From Drug And Alcohol Dependence.”
The ASI, BARC-10, RCS, and SURE measure abstinence from substance use on some level. However, there are different recovery paths, and abstinence from substance use and sobriety is not everyone’s goal for recovery.
Many jurisdictions supported recovery measurement assessments in service settings through staff training
Introducing recovery measurement tools into a variety of settings may present logistical and operational barriers. These include constraints on staff time and availability, insufficient training on how to use the tools effectively, and challenges in aligning these tools with existing clinical workflows or integrating them into electronic health record (EHR) systems. Without adequate support, these barriers can make adoption of recovery-related assessments challenging. Supports such as staff training can help settings integrate and adapt recovery measurement assessments into their service models and provide a mechanism for staff to request additional supports they may need to implement the tool.33 Further, collaborating with outcome-monitoring experts to develop data collection tools can help
service settings track and assess recovery outcomes.34
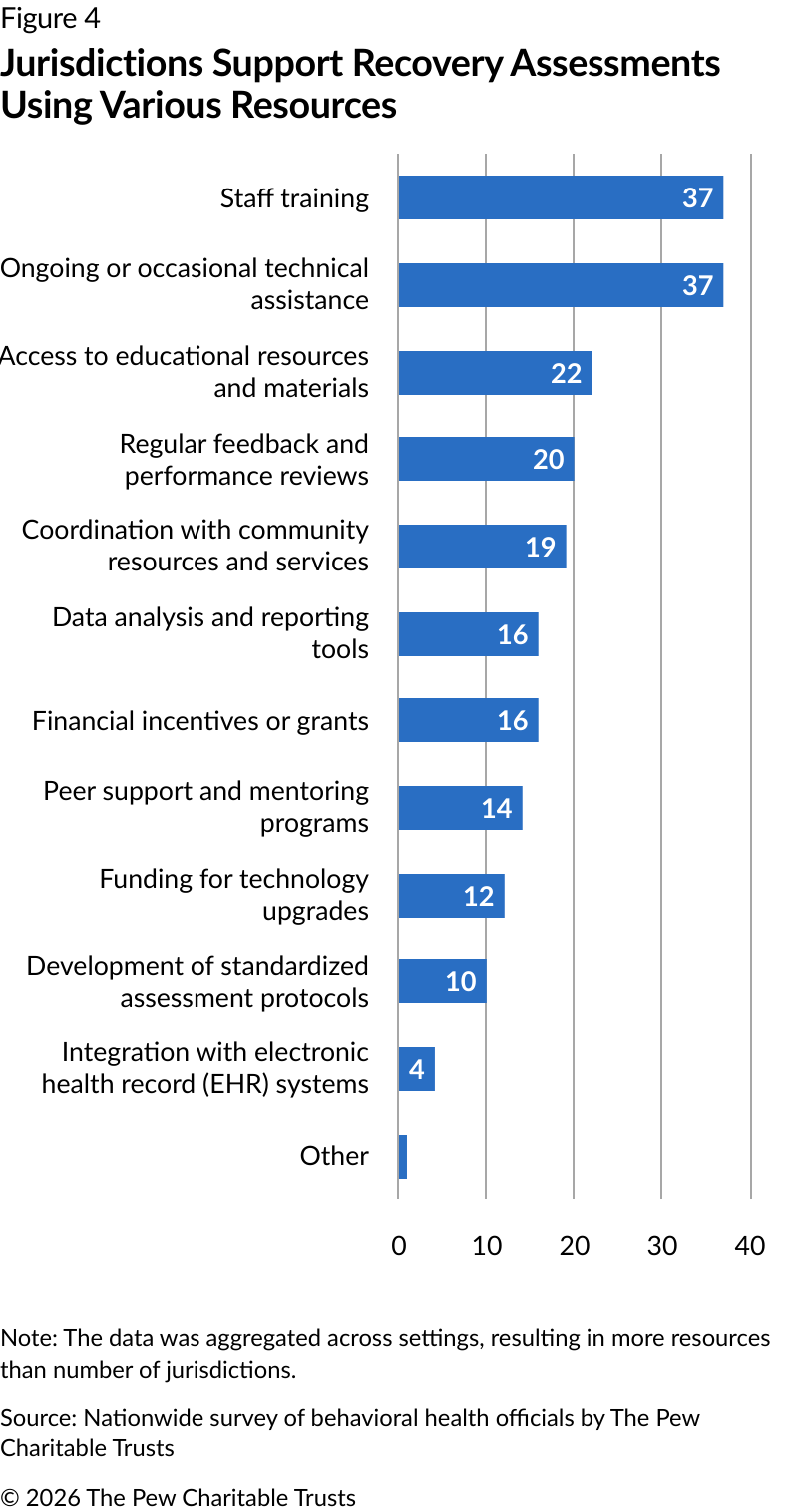
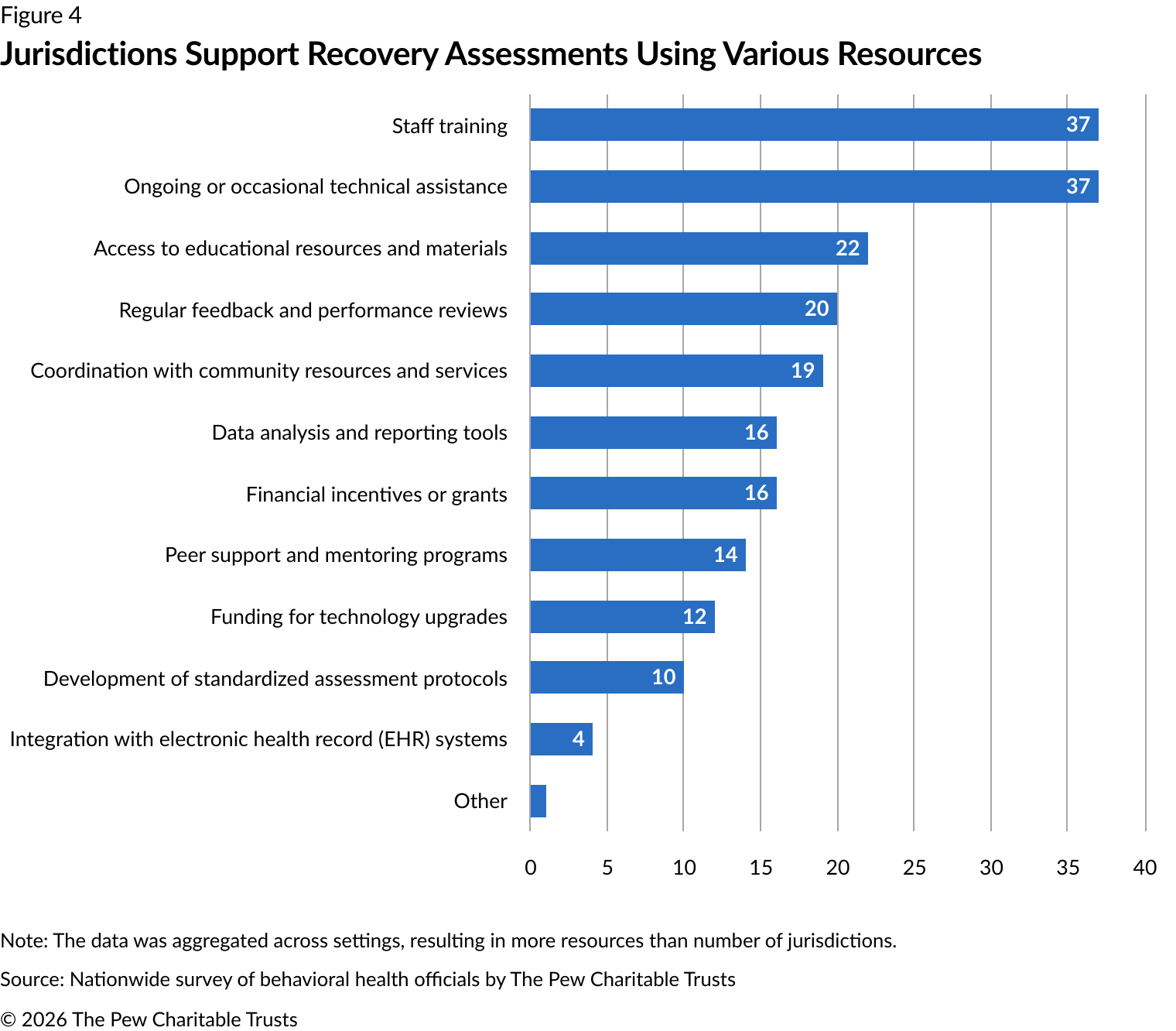
In addition to staff training (37 responses), the most common resources provided across settings included ongoing or occasional technical feedback after initial trainings (37 responses), followed by educational resources (22 responses) and performance reviews (20 responses). Supports related to development of standardized assessment protocols (10 responses) and integration with EHR systems (four responses) were the least provided resources. (See Figure 4.)
Some jurisdictions analyzed recovery measures by demographic variables
Substance use prevalence can vary by race or ethnicity, age, gender, and other demographic variables. For instance, illicit drug use in people age 12 and older was higher among American Indian or Alaska Native people at 29.6% and among multiracial people at 36.2% compared with use by White (27.5%), Black or African American (27.1%), Hispanic (22%), Native Hawaiian and Pacific Islander (18.8%), and Asian (12%) populations in 2024.35 Among people ages 18 to 25, 9.1 million (25.9%) had a substance use disorder in 2024; this rate was the highest among all age groups.36 Among lesbian, gay, or bisexual adults age 18 and over in 2022, 8.1 million (36.5%) reported an SUD, compared with 17.3% of all adults age 18 or older.37
Disaggregating data is crucial to identify and address disparities in treatment, which can affect recovery outcomes. Researchers have found that Black clients and American Indians had a significantly lower likelihood of initiation and engagement in treatment than White clients.38 Among adults who reported ever having a substance use problem, Black respondents were less likely to report being in recovery compared with White populations. This was measured by the response to the question “At this time do you consider yourself to be in recovery or recovered from your own problem with drug or alcohol use”?39
Among officials who responded to the question of whether they disaggregated data based on demographics:
10 analyzed recovery by demographic data at the service setting level while four jurisdictions did not.
Six analyzed recovery by demographics at the population level while four states did not.
Of those jurisdictions that analyzed recovery by demographics, four jurisdictions did so at both the service setting and population level.
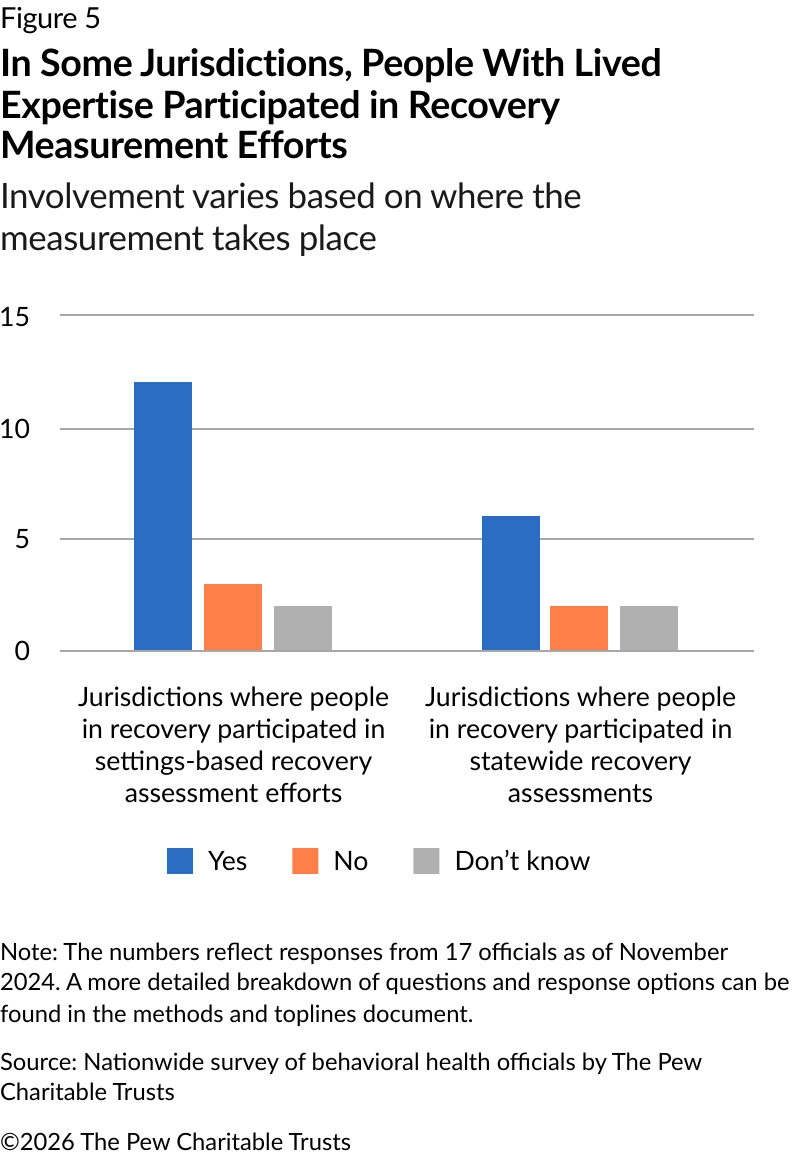
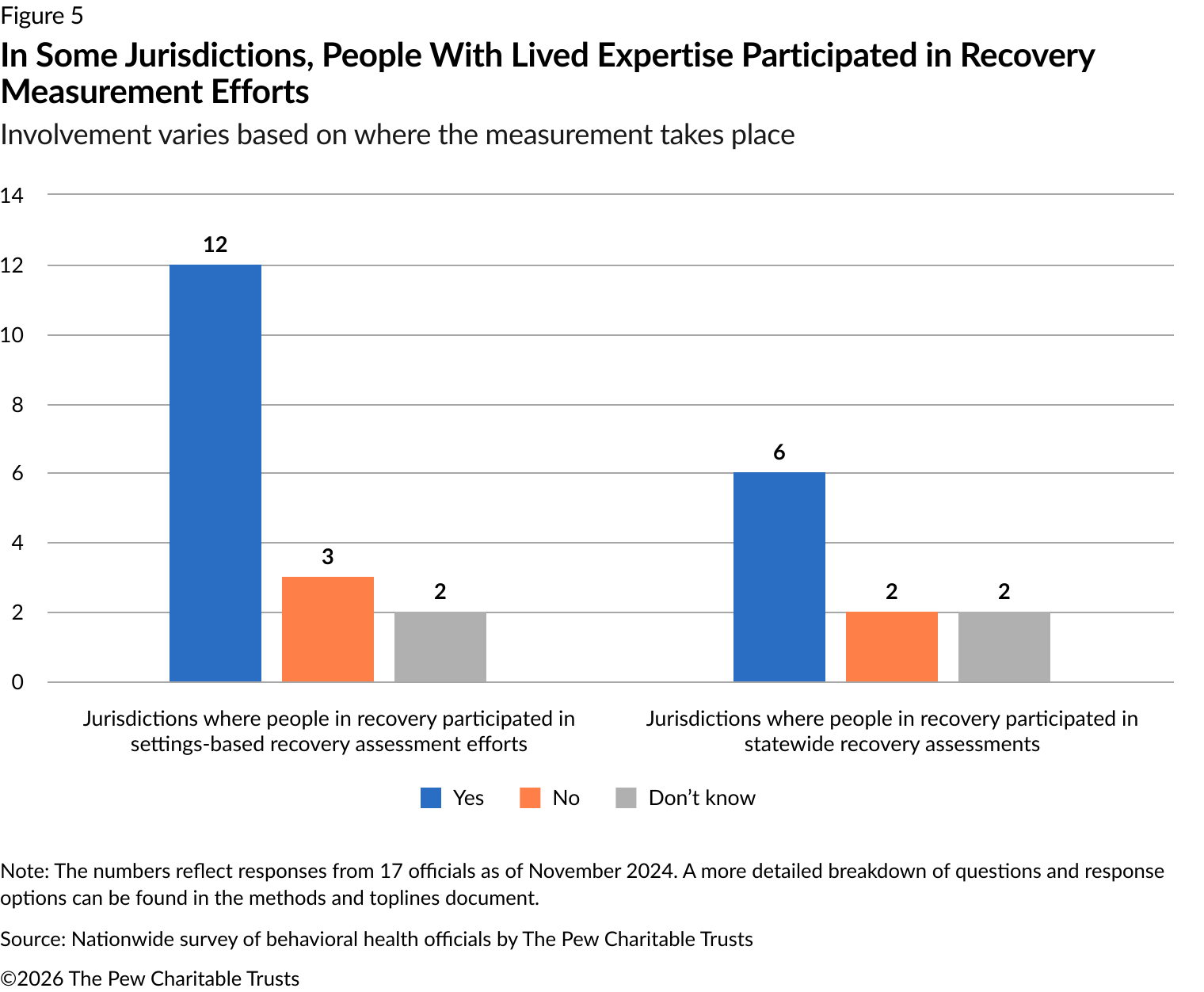
In most jurisdictions, people in recovery participated in measurement efforts
Having people with lived expertise participate in efforts to improve behavioral health service delivery outcomes can help to create systems that are more responsive to community needs.40 People with lived expertise should be involved in developing and refining measures because they can identify relevant outcomes that capture the experience of people in recovery.41 Their participation can improve the relevance and accuracy of data and build trust in the process and promote a sense of ownership among people in recovery.42
Of the jurisdiction officials contacted, 12 of 17 included people in recovery in their efforts requiring certain settings to conduct recovery assessments (Figure 5). Specifically, people with lived expertise were involved in developing measures and recommending recovery assessment tools. As for jurisdiction-wide measurement efforts, people in recovery were included in these initiatives in six jurisdictions. At this level, people in recovery were involved through advisory councils and in planning for identifying recovery metrics.
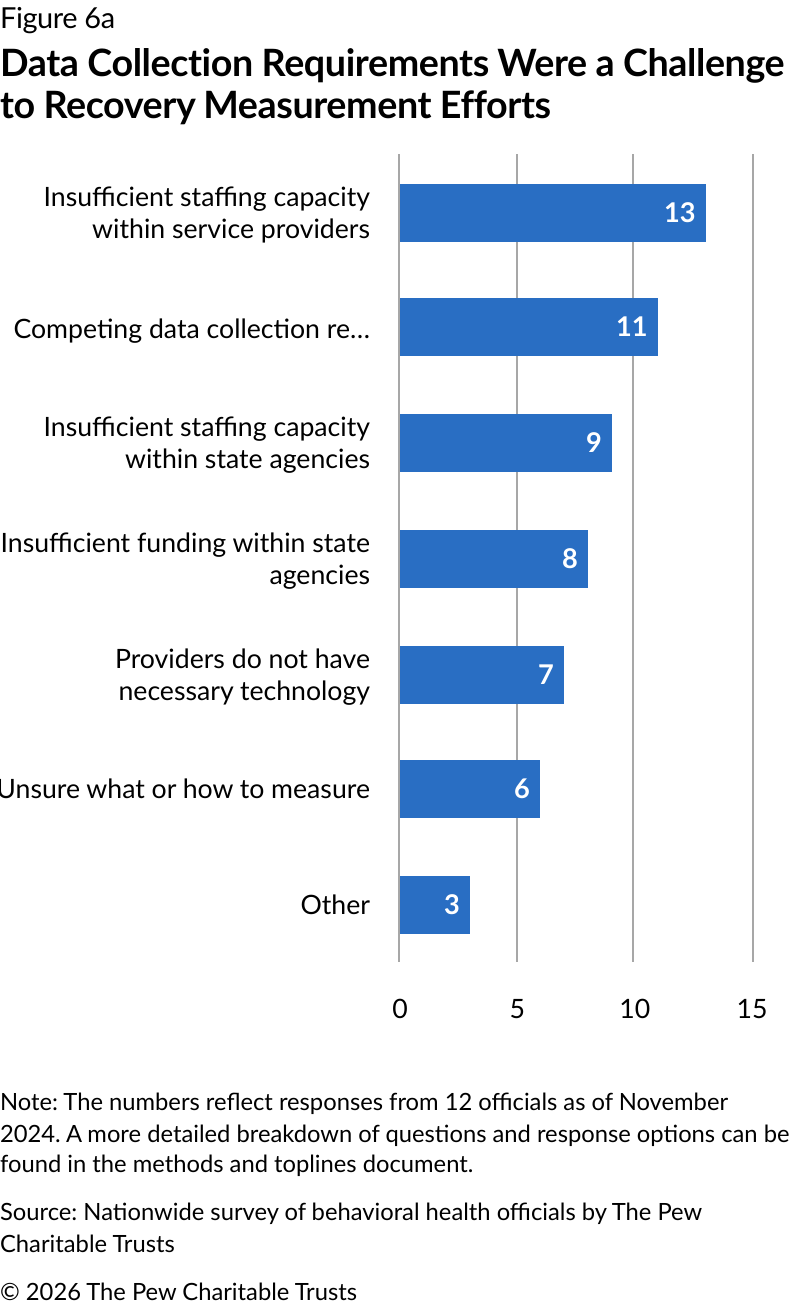
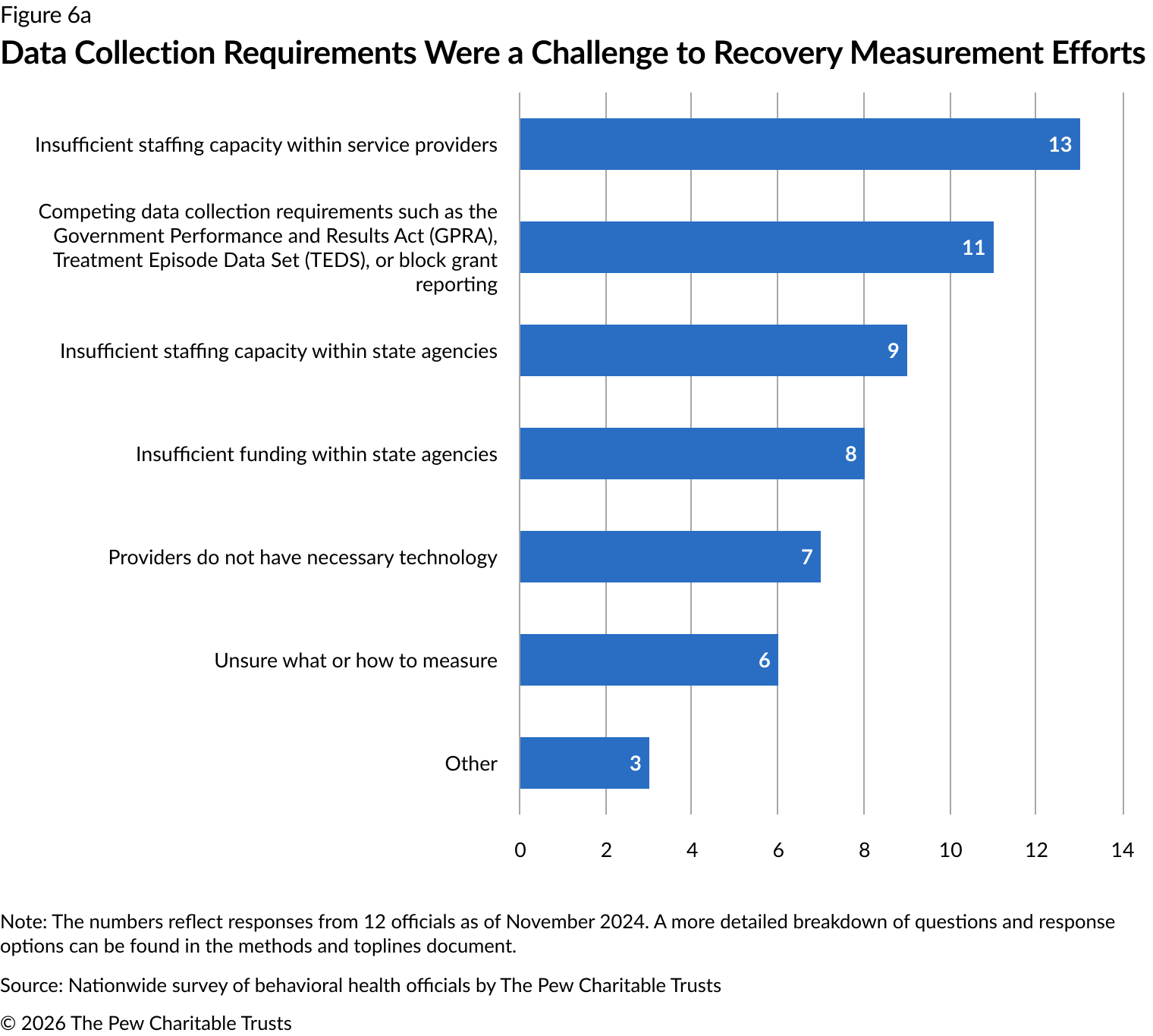
Federal data collection requirements were a challenge to recovery measurement efforts
Among the 18 states that implemented setting-level recovery measurement initiatives, 13 officials reported that insufficient staffing within service settings presented implementation challenges. Competing data collection requirements (11 officials) and insufficient staffing within jurisdiction agencies (nine officials) made up a significant portion of responses as well (Figure 6a).
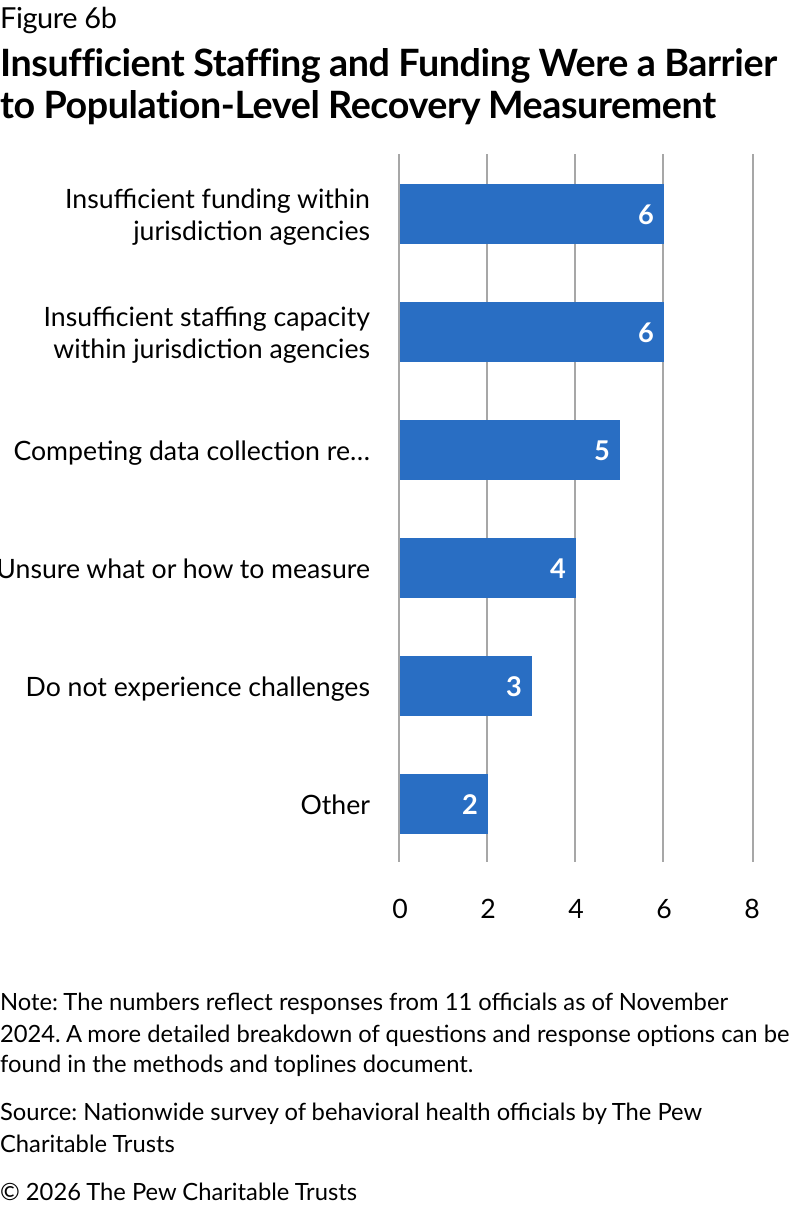
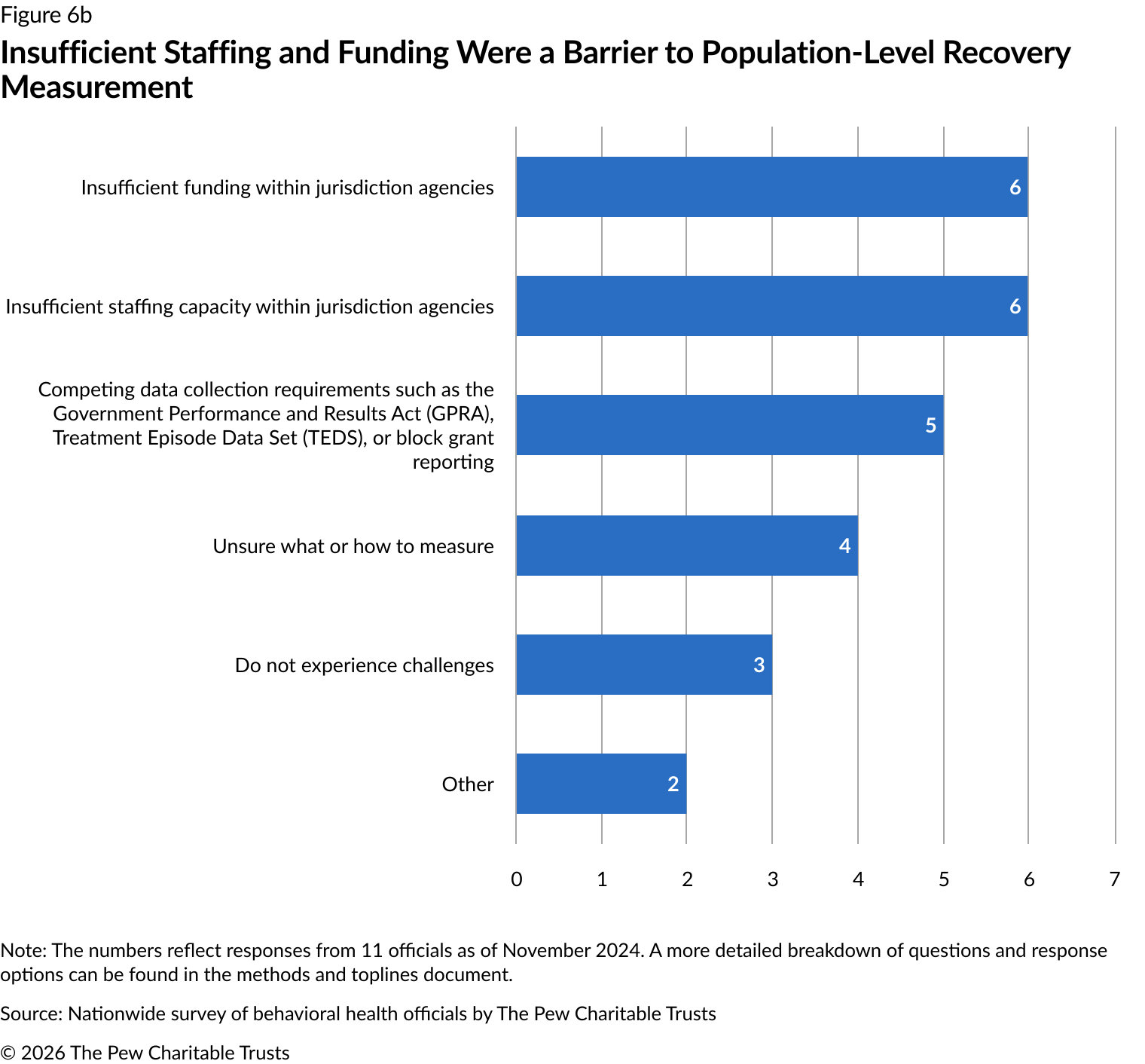
When asked about population-level challenges, officials most commonly reported insufficient staffing and limited funding within state agencies (six each). Meeting federal data collection requirements was the next most commonly reported challenge by five officials (Figure 6b).
Similarly, among the jurisdictions reporting that they do not have any setting-level (13) or population-wide (23) recovery measurement initiatives, common barriers cited included competing federal data collection requirements such as the Government Performance and Results Act (GPRA), Treatment Episode Data Set, or block grant reporting, and insufficient staffing capacity among jurisdiction agencies or service providers.
In response to feedback regarding data collection requirements, SAMHSA has been revising the GPRA to lessen these challenges. This included a request for public comment in the fall of 2024.43
Challenges to measuring recovery at the setting level
Recommendations
By measuring recovery, jurisdiction officials and policymakers can ensure that their care systems support people in achieving their goals. Federal policymakers should streamline data collection requirements to encourage more jurisdictions to adopt recovery measurement initiatives, which can improve care and help policymakers to assess the effectiveness of services.
Engaging people with lived expertise in the design and implementation of these efforts ensures that the measures used are relevant and effective. In addition, disaggregating recovery data collected by demographic variables can inform more targeted interventions.
Conclusion
Pew found that many jurisdictions require service settings to use established measurement tools for recovery assessments while only some measure recovery at a population level or involve people in recovery in these efforts. Jurisdictions not participating in any measurement efforts often decline to do so because they find federal data collection requirements too burdensome for additional initiatives.
While progress is evident, there is a gap in broader jurisdiction adoption of quality measures to enhance recovery services. By implementing measurement initiatives, jurisdictions can strengthen their recovery support systems, improve health outcomes, and enhance the quality of life for people in recovery.
Endnotes
“Recovery and Recovery Support,” Substance Abuse and Mental Health Services Administration, https://www.samhsa.gov/substance-use/recovery.
“Recovery,” National Institute on Drug Abuse, https://nida.nih.gov/research-topics/recovery.
Sarah E. Zemore et al., “Understanding the Shared Meaning of Recovery From Substance Use Disorders: New Findings From the What Is Recovery? Study,” Substance Abuse: Research and Treatment 17 (2023): 1-12, https://doi.org/10.1177/11782218231199372.
Sierra Castedo de Martell et al., “The Cost-Effectiveness of Collegiate Recovery Programs,” Journal of American College Health 72, no. 1 (2024): 82-93, https://doi.org/10.1080/07448481.2021.2024206. David L. Weimer et al., “Net Benefits of Recovery High Schools: Higher Cost but Increased Sobriety and Educational Attainment,” Journal of Mental Health Policy and Economics 22, no. 3 (2019): 109-20, https://pmc.ncbi.nlm.nih.gov/articles/PMC6901088/. Madison Ashworth, David Johnson, and Robin Thompson, “Adaptable Tool for Modeling the Benefits and Costs of Substance Use Disorder Recovery Programs,” Journal of Benefit-Cost Analysis 15, no. 2 (2024): 335-50,
https://www.cambridge.org/core/product/ABB07D30BB83B960554110B2F21E9C35.
Madison Ashworth, David Johnson, and Robin Thompson, “Adaptable Tool for Modeling the Benefits and Costs of Substance Use Disorder Recovery Programs.”
Robert Granfield and William Cloud, Coming Clean: Overcoming Addiction Without Treatment (New York: New York University Press, 1999). David Best and Emily A. Hennessy, “The Science of Recovery Capital: Where Do We Go From Here?,” Addiction 117, no. 4 (2022): 1139-45, https://doi.org/10.1111/add.15732. William Cloud and Robert Granfield, “Conceptualizing Recovery Capital: Expansion of a Theoretical Construct,” Substance Use & Misuse 43, no. 12-13 (2008): 1971-86, https://www.tandfonline.com/doi/abs/10.1080/10826080802289762. Emily A. Hennessy, “Recovery Capital: A Systematic Review of the Literature,” Addiction Research & Theory 25, no. 5 (2017): 349-60,
https://doi.org/10.1080/16066359.2017.1297990.
Integrated Care DC, “Peers Speak Out: Priority Outcomes for Substance Use Treatment & Services,” 2021, https://www.integratedcare.dc.gov/resource/peers-speak-out-priority-outcomes-for-substance-use-treatment-and-services/.
John F. Kelly et al., “‘On Being ‘in Recovery’: A National Study of Prevalence and Correlates of Adopting or Not Adopting a Recovery Identity Among Individuals Resolving Drug and Alcohol Problems,” Psychology of Addictive Behaviors 32, no. 6 (2018): 595-604, https://pubmed.ncbi.nlm.nih.gov/30070538/. Samantha F. Schoenberger et al., “‘My Life Isn’t Defined by Substance Use’: Recovery Perspectives Among Young Adults With Substance Use Disorder,” Journal of General Internal Medicine 37, no. 4 (2022): 816-22, https://doi.org/10.1007/s11606-021-06934-y. David Frank, “‘I Was Not Sick and I Didn’t Need to Recover’: Methadone Maintenance Treatment (MMT) as a Refuge From Criminalization,” Substance Use & Misuse 53, no. 2 (2018): 311-22,
https://doi.org/10.1080/10826084.2017.1310247.
Heather Sophia Lee and Assata Zerai, “‘Everyone Deserves Services No Matter What’: Defining Success in Harm-Reduction-Based Substance User Treatment,” Substance Use & Misuse 45, no. 14 (2010): 2411-27, https://doi.org/10.3109/10826081003712060.
William White and William Cloud, “Recovery Capital: A Primer for Addictions Professionals,” Counselor 9, no. 5 (2008): 22-27, https://www.naadac.org/assets/2416/whitewlcloudw2008_recovery_capital_a_primer.pdf.
“Recovery Capitals,” University of Minnesota: Community-Based Opioid Prevention and Education (C.O.P.E.), https://opioid.umn.edu/recovery-capitals. William White and William Cloud, “Recovery Capital: A Primer for Addictions Professionals.”
Taurmini S.P. Fentress et al., “Dual Study Describing Patient-Driven Harm Reduction Goal-Setting Among People Experiencing Homelessness and Alcohol Use Disorder,” Experimental and Clinical Psychopharmacology 29, no. 3 (2021): 261-71, https://pubmed.ncbi.nlm.nih.gov/34264737/. Heather Sophia Lee and Assata Zerai, “’Everyone Deserves Services No Matter What’: Defining Success in Harm-Reduction-Based Substance User Treatment.”
Mohammad Usama Toseef et al., “Total Cost of Care Associated With Opioid Use Disorder Treatment,” Preventive Medicine 166 (2023): 107345, https://www.sciencedirect.com/science/article/pii/S0091743522003954. Anton L.V. Avanceño et al., “Cost-Effectiveness of Alcohol Use Treatments in Patients With Alcohol-Related Cirrhosis,” Journal of Hepatology 74, no. 6 (2021): 1286-94, https://doi.org/10.1016/j.jhep.2020.12.004. Sarah Callahan, Leonard A. Jason, and Lavome Robinson, “Reducing Economic Disparities for Female Offenders: The Oxford House Model,” Alcoholism Treatment Quarterly 34, no. 3 (2016): 292-302,
https://doi.org/10.1080/07347324.2016.1182814. Sierra Castedo de Martell et al., “The Cost-Effectiveness of Long-Term Post-Treatment Peer Recovery Support Services in the United States,” The American Journal of Drug and Alcohol Abuse 51, no. 2 (2025): 180-90, https://doi.org/10.1080/00952990.2024.2406251.
National Association of Peer Supporters, “National Practice Guidelines for Peer Specialists and Supervisors,” 2019, https://www.peersupportworks.org/wp-content/uploads/2021/07/National-Practice-Guidelines-for-Peer-Specialists-and-Supervisors-1.pdf.
David Eddie et al., “Peer Recovery Support Services and Recovery Coaching for Substance Use Disorder: A Systematic Review,” Current Addiction Reports 12, no. 1 (2025): 40, https://doi.org/10.1007/s40429-025-00645-8.
Sierra Castedo de Martell et al., “What We Know About the Peer Workforce and Economic Evaluation for Peer Recovery Support Services: A Systematic Review,” Substance Use & Addiction Journal 46, no. 1 (2024): 90-102, https://doi.org/10.1177/29767342241281009. “The Potential Economic Benefits of Recovery Coaching,” David Eddie, Recovery Research Institute, June 23, 2025, https://www.recoveryanswers.org/research-post/potential-economic-benefits-recovery-coaching/.
“National Standards for RCOs,” Faces & Voices of Recovery, 2023, https://facesandvoicesofrecovery.org/resource/39801/.
“Alliance for Recovery Centered Organizations (ARCO),” Faces & Voices of Recovery, https://facesandvoicesofrecovery.org/programs/arco/.
National Association of Recovery Residences, “A Primer on Recovery Residences: Frequently Asked Questions,” 2012, https://narronline.org/wp-content/uploads/2024/05/Primer-on-Recovery-Residences.pdf.
Corrie L. Vilsaint et al., “Recovery Housing for Substance Use Disorder: A Systematic Review,” Frontiers in Public Health 13 (2025): https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2025.1506412.
“Medications for Opioid Use Disorder,” National Institute on Drug Abuse, 2025, https://nida.nih.gov/research-topics/medications-opioid-use-disorder.
“Opioid Use Disorder: Treating,” Centers for Disease Control and Prevention, https://www.cdc.gov/overdose-prevention/hcp/clinical-care/opioid-use-disorder-treating.html.
“Substance Use Disorder Treatment Options,” Substance Abuse and Mental Health Services Administration, https://www.samhsa.gov/substance-use/treatment/options. Substance Abuse and Mental Health Services Administration, “Clinical Issues in Intensive Outpatient Treatment,” 2021, https://library.samhsa.gov/sites/default/files/pep20-02-01-021.pdf.
“Screening, Brief Intervention, and Referral to Treatment (SBIRT),” Substance Abuse and Mental Health Services Administration, https://www.samhsa.gov/substance-use/treatment/sbirt.
HIV.gov, “Syringe Services Programs,” https://www.hiv.gov/federal-response/other-topics/syringe-services-programs.
OMNI Institute, “Measuring Peer Outcomes Toolkit: Showing the Impact of Peers in Meaningful Ways,” 2024, https://static1.squarespace.com/static/67017deb9fbcef5ab5aa6989/t/6734b9304772ec02cb3ecd8a/1731508533903/Measuring-Peer-Recovery-Outcomes-Toolkit.pdf. OMNI Institute, “Measuring Outcomes of Peer Recovery Support Services,” 2020, https://www.dropbox.com/scl/fi/1jlmg2kijb5d9eygswfzo/Measuring-Outcomes-of-Peer-Recovery-Support-Services-Lit-Review.pdf?rlkey=8r7cq3lwazlzzdmb0nms1rbyr&e=1&st=x9o4ez5r&dl=0.
OMNI Institute, “Measuring Peer Outcomes Toolkit: Showing the Impact of Peers in Meaningful Ways.” OMNI Institute, “Measuring Outcomes of Peer Recovery Support Services.”
OMNI Institute, “Measuring Peer Outcomes Toolkit: Showing the Impact of Peers in Meaningful Ways.”
Alee Hernandez et al., “Navy Medicine Introduces Value-Based Health Care,” Health Affairs 38, no. 8 (2019): 1393-400, https://doi.org/10.1377/hlthaff.2019.00280. Robert S. Kaplan and Sarah E. Wakeman, “Value-Based Care Can Transform the Treatment of Patients With Substance Use Disorder,” Health Affairs Forefront, Jan. 19, 2024, https://www.healthaffairs.org/content/forefront/value-based-care-can-transform-treatment-patients-substance-use-disorder.
Duke-Margolis Institute for Health Policy, “Addressing Key Barriers to Value-Based Payment for Substance Use Disorder (SUD) Treatment and Recovery: Current Gaps and Opportunities for Advancing Quality Measurement,” 2021, https://healthpolicy.duke.edu/publications/addressing-key-barriers-value-based-payment-substance-use-disorder-sud-treatment-and.
Duke-Margolis Institute for Health Policy, “Addressing Key Barriers to Value-Based Payment for Substance Use Disorder (SUD) Treatment and Recovery: Current Gaps and Opportunities for Advancing Quality Measurement.”
Duke-Margolis Institute for Health Policy, “Addressing Key Barriers to Value-Based Payment for Substance Use Disorder (SUD) Treatment and Recovery: Current Gaps and Opportunities for Advancing Quality Measurement.”
Emily A. Hennessy, Paige Krasnoff, and David Best, “Implementing a Recovery Capital Model Into Therapeutic Courts: Case Study and Lessons Learned,” International Journal of Offender Therapy and Comparative Criminology 69, no. 6-7 (2025): 819-34, https://journals.sagepub.com/doi/abs/10.1177/0306624X231198810.
Mary Jean Costello et al., “The Development and Implementation of an Outcome Monitoring System for Addiction Treatment,” Canadian Journal of Addiction 7, no. 3 (2016): 15-24, https://journals.lww.com/cja/fulltext/2016/09000/the_development_and_implementation_of_an_outcome.3.aspx.
Substance Abuse and Mental Health Services Administration, “Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health,” 2025, https://www.samhsa.gov/data/sites/default/files/reports/rpt56287/2024-nsduh-annual-national-report.pdf.
Substance Abuse and Mental Health Services Administration, “Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health.”
Substance Abuse and Mental Health Services Administration, “2022 National Survey on Drug Use and Health: Among the Lesbian, Gay, or Bisexual (LGB) Population Aged 18 or Older,” 2024, https://web.archive.org/web/20250116000835/https:/www.samhsa.gov/data/sites/default/files/reports/rpt44472/2022-nsduh-pop-slides-lgb.pdf.
Andrea Acevedo et al., “Disparities in the Treatment of Substance Use Disorders: Does Where You Live Matter?,” Journal of Behavioral Health Services and Research 45, no. 4 (2018): 533-49, https://pmc.ncbi.nlm.nih.gov/articles/PMC6087681/.
Christopher M. Jones, Rita K. Noonan, and Wilson M. Compton, “Prevalence and Correlates of Ever Having a Substance Use Problem and Substance Use Recovery Status among Adults in the United States, 2018,” Drug and Alcohol Dependence 214 (2020): 108169, https://pubmed.ncbi.nlm.nih.gov/32682218/.
Natasha Y. Sheikhan et al., “Exploring the Impact of Engagement in Mental Health and Substance Use Research: A Scoping Review and Thematic Analysis,” Health Expectations 26, no. 5 (2023): 1806-19, https://pubmed.ncbi.nlm.nih.gov/37282732/.
Elizabeth Okrant, Sharon Reif, and Constance M. Horgan, “Development of an Addiction Recovery Patient-Reported Outcome Measure: Response to Addiction Recovery (R2AR),” Substance Abuse Treatment, Prevention, and Policy 18, no. 1 (2023): 52, https://pubmed.ncbi.nlm.nih.gov/37658373/.
Ashley Jasko and Dana Foglesong, “Meaningfully Engaging People With Lived Experience in Behavioral Health Reform: A Guide for States,” Center for Health Care Strategies, 2025, https://www.chcs.org/resource/meaningfully-engaging-people-with-lived-experience-in-behavioral-health-reform-a-guide-for-states/. Christopher Menschner and Amy Brinkley, “What We Measure Matters: Centering Lived Experience in Developing Behavioral Health Quality Measures,” Center for Health Care Strategies, 2024, https://www.chcs.org/resource/what-we-measure-matters-centering-lived-experience-in-developing-behavioral-health-quality-measures/.
Substance Abuse and Mental Health Services Administration, Agency Information Collection Activities: Proposed Collection; Comment Request; Correction, Fed. Reg. (Sept. 6, 2024), https://www.federalregister.gov/d/2024-20051.