
Global physical activity inequalities
The main results of the global, domain-specific physical activity inequalities analysis are shown in Figs. 1–3, Extended Data Fig. 1 and the Supplementary Information.
Fig. 1: Domain-specific physical activity prevalence by country income categories.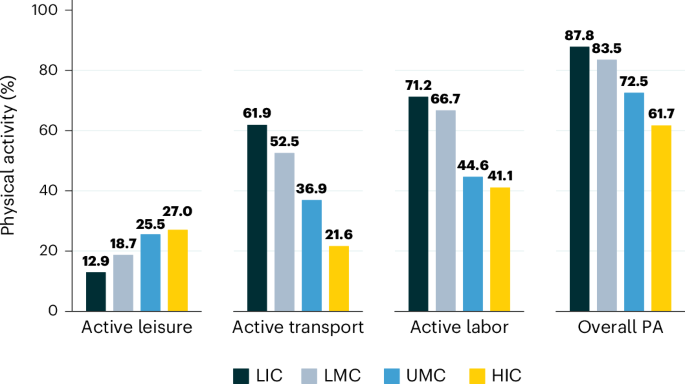
Percentage of the population meeting WHO Physical Activity Guidelines with leisure-specific, transport-specific, labor-specific and overall (all domains) moderate-to-vigorous-intensity physical activity, by World Bank country income categories (LIC, low-income country; LMC, lower middle-income country; UMC, upper middle-income country; HIC, high-income country) (source data: WHO STEPS, n = 68 countries; prevalence data date range: 2008−2019). PA, physical activity.
Fig. 2: Socioeconomic and gender-based domain-specific physical activity inequalities by country income category.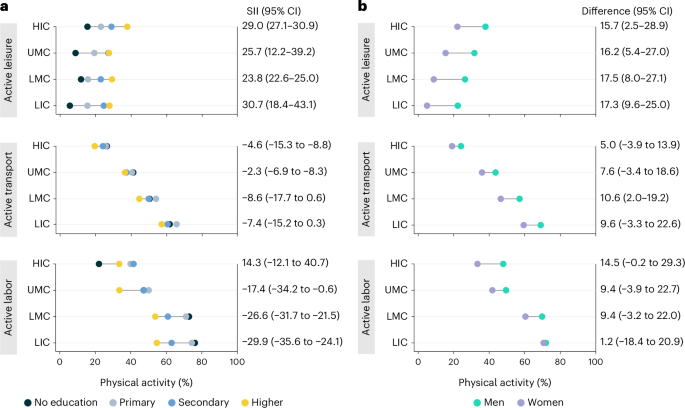
Unidimensional socioeconomic (education used as proxy) (a) and gender-based (b) inequalities in prevalence of meeting WHO Physical Activity Guidelines through leisure time (active leisure), transport-related (active transport) and occupational (active labor) physical activity by World Bank country income categories (LIC, low-income country; LMC, lower middle-income country; UMC, upper middle-income country; HIC, high-income country). In a, SII (slope index) denotes the absolute differences in predicted values (percentage points) between those with the highest versus lowest educational attainment, taking into consideration the entire distribution of education in the population, by using a logistic regression model. In b, ‘Difference’ denotes absolute differences in percentage points between men and women (source data: WHO STEPS, n = 68 countries; prevalence data date range: 2008−2019). CI, confidence interval.
Fig. 3: Intersectional analysis of socioeconomic and gender-based inequalities in domain-specific physical activity, by country income group.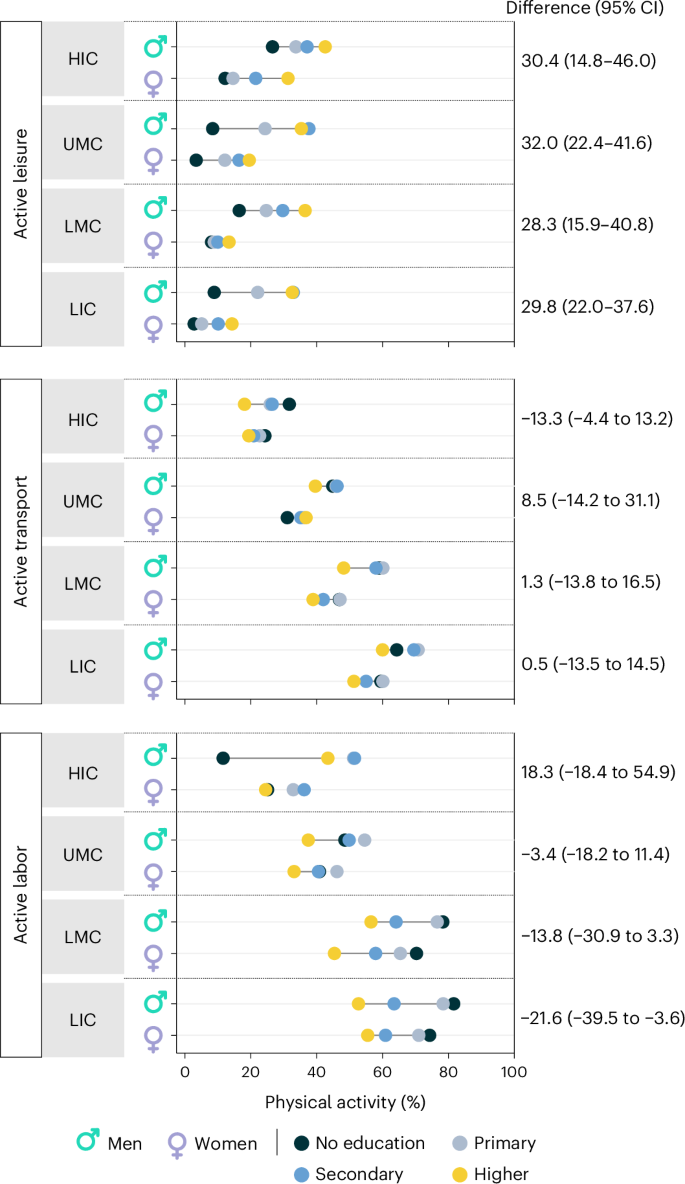
Multidimensional gender and socioeconomic (education as proxy) inequalities in prevalence of meeting WHO Physical Activity Guidelines through leisure time (active leisure), transport-related (active transport) and occupational (active labor) physical activity, by World Bank country income categories (LIC, low-income country; LMC, lower middle-income country; UMC, upper middle-income country; HIC, high-income country). The ‘Difference’ column denotes the absolute difference in percentage points between men of the highest socioeconomic strata and women of the lowest socioeconomic strata (source data: WHO STEPS, n = 48 countries; prevalence data date range: 2008−2019). CI, confidence interval.
This analysis was informed by three theoretical frameworks or concepts: (1) physical activity security, (2) necessity-based versus choice-based physical activity and (3) intersectionality. The concept of ‘physical activity security’ aims to elevate physical activity access as a human right and has been defined as ‘when all people, at all times, have physical and economic access to sufficient, safe, and enjoyable physical activity to meet not only their health needs, but to promote physical and emotional well-being and social connectedness, for an active and healthy life’14.
Complementarily, the necessity-based versus choice-based physical activity framework posits that, for many worldwide, a major driver of physical activity is economic necessity rather than free, non-economically coercive healthy choices15. As a consequence, a large portion of global physical activity takes place in the occupational and transport domains and, for many, occurs in suboptimal conditions for health, safety and wellbeing (for example, having to travel long distances by foot in unsafe environments and forced or not entirely safe labor conditions). Thus, despite high levels of overall physical activity, globally, many people remain ‘physical activity insecure’. Thus, the necessity-based versus choice-based physical activity framework calls into question the ethics of assuming all physical activity as being supportive of optimal physical, mental and social wellbeing. Importantly, this framework does not deny the well-documented positive effects of overall physical activity on cardiometabolic health and all-cause mortality, but, rather, it adopts a holistic definition of health, aligned with that of the WHO7.
Finally, intersectionality theory is rooted in the US Black feminist movement16, underscoring that ‘human experience is jointly shaped by multiple social positions (for example, race, gender), and cannot be adequately understood by considering social positions independently’17. Intersectionality recognizes the interdependent and interactive nature of systems of oppression in societies (for example, structural racism, sexism, gender-based discrimination, ableism, etc.) and their interwoven impacts on individuals belonging to not one but multiple groups disadvantaged by societal norms, systems and policies.
Together, these theoretical concepts and frameworks motivated our examination of the relative contribution to overall physical activity of three domains: active leisure, primarily associated with choice-based physical activity; active labor, primarily associated with economic necessity; and active transport, which, depending on its environmental and societal context, can result from free, non-coercive choices or from economic necessity. We hypothesized that more socially advantaged individuals based on status-conferring characteristics (that is, men, people of high socioeconomic status and residents of high-income countries) would have greater access to choice-based physical activity. Furthermore, we hypothesized that the intersection of multiple social status-conferring elements (gender, socioeconomic status and country of residence) could lead to magnified inequalities in domain-specific physical activity.
Socioeconomic physical activity inequalities
We found evidence of both within-country and between-country socioeconomic inequalities across physical activity domains. Figure 1 shows that when considering overall levels of physical activity (that is, occurring in any domain), the higher the World Bank country income category, the lower the prevalence of meeting physical activity guidelines, with the prevalence difference between the high-income versus low-income World Bank country income categories of −26.1 percentage points (pp). This could be interpreted as suggestive that physical inactivity is a major public health problem only in wealthy nations. However, domain-specific findings reveal a more complex scenario. Generally, the higher the World Bank country income category, the higher the prevalence of meeting guidelines with active leisure, whereas the lower the World Bank country income category, the higher the prevalence of meeting guidelines through active transport and active labor. Between-country income grouping inequalities were wider for physical activity domains in which necessity-based physical activity takes place (active labor and, in many contexts, active transport) than for active leisure (always choice based). The prevalence difference between the high-income versus low-income country categories was of −40.3 pp for active transport and of −30.1 pp for active labor. In addition, the prevalence difference between the high-income versus low-income country categories for active leisure was of 14.1 pp. Furthermore, when examining the proportional contribution of physical activity by domain to overall physical activity by country income level (Extended Data Fig. 1), the same pattern becomes apparent: the higher the country income level, the higher the contribution of choice-based physical activity (active leisure). In low-income and lower middle-income countries, less than 10% of overall physical activity derives from active leisure, contrasting with high-income countries where over 30% of overall physical activity corresponds to active leisure.
Findings from the within-country analysis of socioeconomic inequalities (Fig. 2a) show that the prevalence of meeting physical activity guidelines through active leisure was approximately 20 pp higher among individuals of high versus low socioeconomic status (median slope index of inequality (SII) = 19.5, SII min = −18.8, SII max = 46.1, SII range = 64.9). Inequalities of similar magnitude were observed across World Bank country income categories (Fig. 3a), emphasizing that unequal access to active leisure exists across societies, including in wealthy countries. Across all country income categories, lower prevalence of meeting guidelines through active transport was observed among those of higher socioeconomic status relative to those of lower socioeconomic status, although higher variability in socioeconomic inequalities was observed across countries for this domain (median SII = −4.8, SII min = −34.9, SII max = 39.7, SII range = 74.6). The widest within-country socioeconomic inequalities were observed in the occupational domain, with the prevalence of meeting physical activity guidelines through active labor being approximately 16 pp higher among individuals with no formal education compared to those with high educational attainment (median SII = −16.1, SII min = −37.4, SII max = 12.2, SII range = 28.6).
Gender-based physical activity inequalities
Within-country findings show that across domains and country income categories, the prevalence of meeting physical activity guidelines was higher among men than among women (Fig. 2b). For active leisure, the prevalence was 15 pp lower among women versus men (median difference = 15.4, difference min = −16.8, difference max = 36.1, difference range = 52.9), with the active leisure gender gap being similar in magnitude regardless of macroeconomic country context (Fig. 3b). Notably, the prevalence of meeting guidelines with active leisure was similar among women in high-income countries and men in low-income countries. Patterns for active transport and active labor were similar. The prevalence of meeting guidelines through either active transport or active labor was approximately 8 pp higher for men versus women (active transport: median difference = 7.6, difference min = −14.5, difference max = 47.9, difference range = 62.4; active labor: median difference = 8.0, difference min = −10.0, difference max = 27.8, difference range = 38.8). The active transport gender gap was smaller in high-income countries than in all other country income categories (that is, LMICs). In addition, the active labor gender gap was widest in high-income countries and virtually absent in low-income countries.
Country-level estimates of socioeconomic and gender-based inequalities in active leisure, transport and labor for the 68 WHO STEPS countries are available in the Supplementary Information.
Socioeconomic and gender-based inequalities: an intersectionality approach
In addition to the unidimensional analysis of socioeconomic-based and gender-based physical activity inequalities, we assessed physical activity inequalities at the intersection of these two social identities. When comparing the wealthiest men to the poorest women within countries, we observed an absolute difference of approximately 28 pp for meeting physical activity guidelines through active leisure. The gap in active leisure between wealthy men and poor women is similar across country income categories and is wider than the gap observed in the unidimensional analysis for gender-based inequalities. When adding the dimension of macroeconomic country context, by contrasting wealthy men in rich nations with the most socioeconomically disadvantaged women in poor nations, the estimated gap became 40 pp.
Different inequality patterns were observed for active transport and active labor, with large variations in the degree of inequality between wealthy men and poor women across country income categories (Fig. 3). For instance, in high-income and upper middle-income countries, more women of low socioeconomic status meet guidelines through active transport than wealthy men, but smaller differences are observed in lower middle-income and low-income countries. Likewise, in all country income groups except high-income countries (that is, in LMICs), the prevalence of meeting guidelines through active labor is higher in women of low socioeconomic status than in men of high socioeconomic status.
Health benefits of physical activity beyond cardiometabolic health
In addition to pervasive inequalities and the obesity and cardiometabolic disease crises that many countries are undergoing, infectious disease emergencies, mental health disorders and high mortality and morbidity due to cancer are common elements of 21st century syndemics3,18,19. The sections below summarize findings of three narrative reviews on the connections of physical activity with immunity and infectious diseases, depression and cancer.
Physical activity, immunity and infectious diseases
It has been argued that the importance of physical activity in immune function for preventing and mitigating infections has been underestimated by scientific consensus groups20, despite growing evidence linking physical activity to reduced infection risk and enhanced immunity.
Regular moderate-to-vigorous physical activity boosts immune responses to vaccines, reduces viral loads, lowers inflammation, enhances peripheral immune cell function and increases survival in mice challenged with respiratory pathogens (for example, influenza)21. Physical activity enhances immunity through three key biological pathways (Fig. 4): (1) increased immune surveillance21,22,23,24,25—the body’s natural defence mechanism, continuously monitoring and recognizing abnormal cells or foreign invaders; (2) favorable immune system remodeling25,26,27,28—the dynamic process of alterations within the immune system due to aging or stress or in response to infections, with physical activity promoting more youthful phenotypes associated with improved immune response; and (3) inflammation reduction25,29,30—physical activity can directly and indirectly reduce chronic inflammation by altering the phenotype and function of inflammatory immune cells and by reducing highly inflammatory white adipose tissue, respectively.
Fig. 4: The three main known pathways by which physical activity enhances immunity.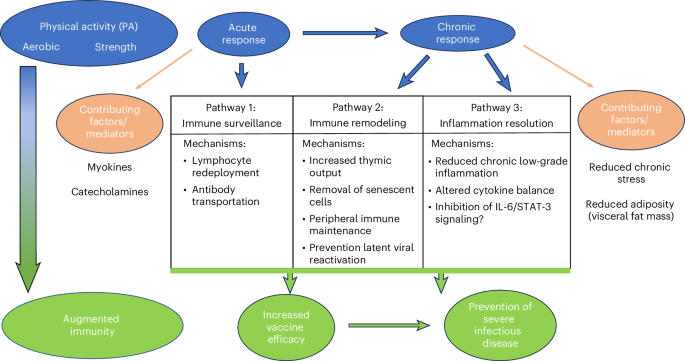
Physical activity augments immunity by increasing vaccine efficacy and preventing severe infectious disease outcomes. Known pathways include improvements in (1) immune surveillance (acute response), (2) immune remodeling (chronic response) and (3) inflammation resolution (chronic response).
Epidemiological evidence aligns with mechanistic research. Findings from population-based studies conducted during the COVID-19 pandemic support that physical activity participation at recommended levels12 is associated with lower risks of COVID-19-related health outcomes. In a meta-analysis of 16 studies including more than 1.8 million adults, regularly active individuals, compared to those inactive prior to infection, experienced the following: (1) 11% lower risk of COVID-19 infection (relative risk = 0.89, 95% confidence interval: 0.84−0.95); (2) 36% lower risk of hospitalization (relative risk = 0.64, 95% confidence interval: 0.54−0.76); (3) 34% lower risk of severe COVID-19 illness (relative risk = 0.66, 95% confidence interval: 0.58−0.76); and (4) 43% reduction in COVID-19-related mortality (relative risk = 0.57, 95% confidence interval: 0.46−0.71)31. When examining physical activity as a continuous measure with risk of severe disease, the dose−response curve showed a sharp reduction in risk until the equivalent of 150 minutes per week of activity, with lesser risk reduction/plateauing thereafter. The associations of physical activity with lower risks of severe COVID-19 outcomes appear consistent across age, sex, race/ethnicity, body mass index and preexisting cardiovascular disease32,33.
Physical activity and mental health
Depression is among the most pressing mental health issues globally34. A large body of research has examined the links between physical activity and depression, with over 150 systematic reviews with meta-analysis found through May 2024 (Supplementary Information).
The available evidence supports that physical activity can help prevent and attenuate depression and depressive symptoms among adults, adolescents and older adults. A recent (2022) harmonized meta-analysis of 15 prospective cohort studies summing more than 12 million person-years of follow-up assessed the effect of non-occupational physical activity on incident depression among adults and reported evidence of an inverse curvilinear association: accumulating half of the recommended amount of physical activity was associated with an 18% lower incidence of depression (95% confidence interval: 13−23), and meeting guidelines was associated with a 25% (95% confidence interval: 18−32) lower incidence35. The associations appeared similar across gender and age groups. In another meta-analysis of prospective cohort studies36, inverse associations of physical activity with depressive symptoms were reported for adolescents and young adults (odds ratio = 0.90, 95% confidence interval: 0.83−0.98) and for older adults (odds ratio = 0.79, 95% confidence interval: 0.72−0.86).
Evidence also supports physical activity as a promising treatment for depression. A 2024 meta-analysis summarized findings from 218 randomized controlled trials (RCTs) with a combined total of 14,170 participants with major depressive disorder37. Findings support that physical activity across a variety of modalities (walking and jogging, yoga, strength training, mixed aerobic exercises, tai chi or qigong) has moderate yet clinically significant effects in reducing depressive symptoms relative to controls. Although similarly large meta-analyses of RCTs are lacking for youth, the available evidence is consistent with that of adults38.
Physical activity and cancer
Cancer is the second leading cause of death worldwide, with over 10 million cancer deaths in 2023 (ref. 39). The link between physical activity and cancer prevention and control has long been established.
Multiple large-scale reviews of epidemiological studies consistently report higher levels of active leisure, non-occupational or overall aerobic physical activity being associated with lower risk of several types of cancer. Findings from a recent (2019) and robust systematic review show that people with the highest versus the lowest levels of aerobic physical activity have risk reductions of approximately 10−20% for multiple site-specific cancers, including breast, colorectal, bladder, endometrial, esophageal, renal and gastric cancers40. Furthermore, a 2025 review identified individual studies published since 2019 reporting consistent findings41. With respect to muscle-strengthening physical activity, a 2021 review found a significant association between high (versus low) levels of muscle-strengthening activity and a 26% lower risk of renal cancer (hazard ratio = 0.74; 95% confidence interval: 0.56−0.98)42. However, this evidence was drawn from only two studies. More work is needed assessing the possible independent or cumulative contributions of muscle-strengthening activity to cancer prevention, beyond or compounded with those of aerobic physical activity.
Regarding survival among people diagnosed with cancer, a high-quality systematic review published in 2020 (ref. 43) found compelling evidence from 136 studies supporting higher survival among patients with cancer in the highest versus lowest categories of physical activity. This review assessed the association of both pre-diagnosis and post-diagnosis physical activity with cancer mortality (all sites), with reports of significant mortality risk reductions for both physical activity assessments. A higher risk reduction was observed for post-diagnosis physical activity (37% lower cancer mortality risk among the highest versus lowest activity group; hazard ratio = 0.63, 95% confidence interval: 0.53−0.75) than for pre-diagnosis physical activity (18% lower risk among the highest versus lowest activity group; hazard ratio = 0.82, 95% confidence interval: 0.79−0.86). The authors report similar associations across 11 individual cancer types examined. Notably, these findings were consistent across multiple population subgroups, including by sex, body mass index, menopausal status and colorectal cancer subtype and for both active leisure and overall physical activity levels. These results were recently ratified by a new, large-scale multicenter RCT that tested the effects of a structured exercise intervention after chemotherapy on colon cancer survival outcomes44. However, a systematic review by Takemura et al.45 focused on patients with advanced cancer found weak evidence supporting a protective role of physical activity for mortality risk reduction. This could suggest that the benefits of post-diagnosis physical activity for cancer survival are limited to patients with early-stage or mid-stage cancer, but more research is needed that differentiates the effects of physical activity among patients with advanced cancer with a terminal versus a non-terminal diagnosis.
Although most evidence linking physical activity to cancer outcomes has focused on overall or leisure time physical activity, results from a new, large-scale prospective study of occupational physical activity show that, although active labor may lower the incidence of some cancers, it is also associated with a higher mortality from other cancer types46. It is worth noting that the field of physical activity oncology has also begun to emphasize the effect of physical activity for improving additional outcomes among cancer survivors and patients with advanced cancer, including muscle strength, mental health and quality of life, as well as the possible role of physical activity as an enhancer of cancer treatment47. The Supplementary Information provides an extended summary of the evidence linking physical activity to cancer-related outcomes.
Reconceptualizing physical activity for public health in the 21st century
Drawing on lessons from the global analysis of physical activity inequalities and of the critical review of evidence pointing toward multiple health benefits of physical activity for disease prevention and control, we propose shifting from the current physical activity research and practice model anchored on obesity and cardiometabolic disease prevention and management (Fig. 5a) toward one that recognizes the broader role of physical activity for multiple public health and societal priorities. The new model explicitly recognizes the influences of social status-conferring identities, broad societal context (including physical activity policy and political economies, addressed in detail in Series Paper 3 (ref. 48)) and planetary-level factors (Series Paper 2 (ref. 49)) on the circumstances in which activity occurs and, ultimately, on individual and population patterns of physical activity (Fig. 5b). The top part of the model is informed by the Dahlgren−Whitehead Social Determinants of Health model50 and by the findings of our global inequalities/intersectionality analysis. The bottom section is informed by our review of the less-recognized benefits of physical activity for health and wellbeing. The model highlights the bidirectional relationship between the health status of populations and their physical activity patterns plus broader contextual elements. Finally, informed by our global analysis of physical activity inequalities and their theoretical precursors (physical activity security, the necessity-based versus choice-based physical activity framework and intersectionality theory), the proposed reconceptualization posits centering public health research and promotion on the concept of ‘physical activity for health and wellbeing’. Table 1 presents the four main elements of this reconceptualization, including recommendations for physical activity surveillance, research and promotion.
Fig. 5: Toward a reconceptualized framework of physical activity for public health in the 21st century.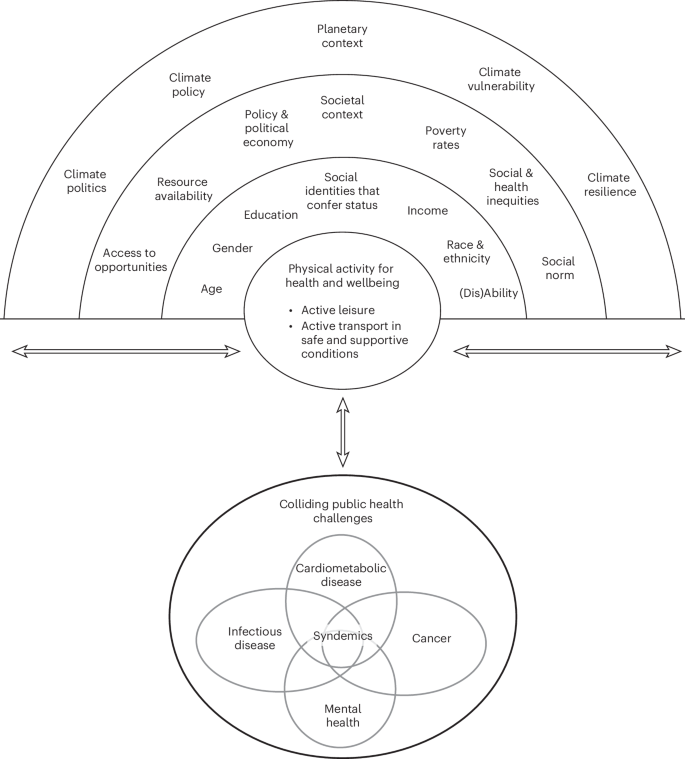
A proposal to shift from the current conceptualization of the public health relevance of physical activity, centered on cardiometabolic disease prevention and management (a), toward a reconceptualized understanding of physical activity for public health research, policy and practice in the 21st century, centered on ‘physical activity for health and wellbeing’ (b).
Table 1 Reconceptualization of physical activity for public health in the 21st century