
Ethical approval
This study complies with all relevant ethical regulations. We have received ethical approval from the South Central Oxford C Research Ethics Committee (REC) for use of the CRIS system as a secondary research database (REC reference: 23/SC/0257). This study received approval by CRIS (reference: 22-040) on 8 June 2022 (including external data linkages). Consent was not needed as we used a secondary research database.
Study design
This is a retrospective cohort study using an exposure–outcome design investigating the relationship between primary care consultation modalities, categorized as face to face and remote (via telephone, text, email and video calls), and acute mental health service use. Specifically, it examines the number of emergency contacts with mental health liaison teams, psychiatric hospital admissions, inpatient bed-days and involuntary MHA admissions among patients with depression, anxiety and SMI (including bipolar and psychotic disorders) residing in a specific geographic catchment area, the London borough of Lambeth, before and during the COVID-19 pandemic. In this UK-based study, emergency contacts with mental health liaison teams refer to contacts in Accident and Emergency (A&E) departments of general hospitals that required intervention from mental health teams and were consequently recorded in the electronic health records of the mental health service.
Data sources
This study utilized data from the CRIS system, which extracts predefined search parameters from the electronic patient records of the SLaM NHS Trust, a major mental health care provider covering a defined geographic catchment area across four London boroughs (Croydon, Lambeth, Lewisham and Southwark; approximately 1.3 million residents), which has deployed fully electronic health records across all services since 2006. CRIS provides researchers access to de-identified data from these records within a robust data governance and security framework36,37. Since the development of the platform in 2007–2008, CRIS data have been linked to a range of external data sources, including, as in this study, to primary care consultation data from the London borough of Lambeth, stored within the LDN38 via a bespoke trusted research environment administered by SLaM’s Clinical Data Linkage Service36,37. The linkage between LDN and CRIS has been previously used to investigate health inequalities and service use pathways9,33. Of relevance to this study, Lambeth represents around one quarter of SLaM’s catchment population and all of Lambeth’s catchment receives public mental health services from SLaM.
Study population and case definition
The study cohort included patients registered with an LDN GP within the study period (1 January 2019 to 31 December 2021) who had a diagnosis of anxiety, depression or SMI, including bipolar and psychotic disorders, according to the Systematized Nomenclature of Medicine Clinical Terms (SNOMED), a structured clinical vocabulary used in electronic health records. Patients were excluded if they were under 18 years of age at exposure, were not registered to a GP or received zero consultations during the exposure period, or died before the start of the outcome period.
The study period was divided into five exposure–outcome subperiods, equally distributed over the full timeline (Fig. 1). Each exposure period was of 6 months in length. We calculated ‘active days’, defined as the number of days the patient was registered with a GP during this window. The exposure metric was the proportion of remote GP consultations experienced during that time, which was calculated as the number of remote GP consultations divided by the total number of GP consultations with valid (nonmissing) modalities. At the end of each exposure subperiod, the outcome measures were then calculated for each patient in the subsequent 6-month outcome period, adjusting for ‘days at risk’, which restricted the number of follow-up days if the patient died during the outcome phase.
Fig. 1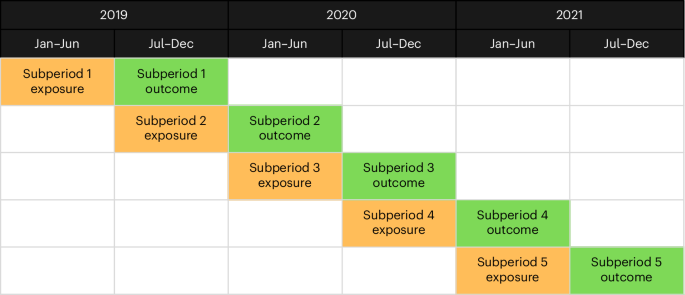
The five exposure–outcome subperiods, distributed across the full study period.
The data from each exposure–outcome subperiod were then recombined. If a patient featured in more than one eligible subperiod, only one set of their data was used in the recombination, selected by random. The associated subperiod for each final patient was recorded for future use when adjusting for confounders, allowing mitigation of the effect of the pandemic peaks.
Variables and outcome measures
The primary outcome measures were the number of: (1) emergency contacts with mental health liaison teams, (2) psychiatric hospital admissions, (3) inpatient bed-days and (4) involuntary admissions under the MHA, as recorded in mental healthcare (CRIS). Inpatient bed-days were calculated within each outcome period, and admission episodes extending beyond the end of the period were truncated. For the final outcome, we counted admissions that were classified as compulsory detention under the MHA at the time of admission.
In addition, the following data were extracted for each patient, using the most recent records at the time of extraction: date of death, age, sex, ethnicity, neighborhood socioeconomic deprivation (measured by the IMD), history of depression, anxiety or SMI (including bipolar and psychotic disorders) according to SNOMED, admission date, discharge date, GP consultation date and GP consultation modality.
Missing data handling
Patterns of missing data were examined at patient and GP-practice levels. Missingness was associated with observed characteristics, including demographic and practice-level data recording practices, supporting a missing-at-random assumption. MICE was used to address incomplete data for sex, ethnicity, IMD and proportion of remote consultations, generating five imputed datasets that incorporated all analytical variables. Estimates from the imputed datasets were pooled using Rubin’s rules.
Data analysis
The analyses were performed within a Jupyter Notebook using Python (version 3.11) with the statsmodels (version 0.14.0) and SciPy (version 1.16.2) packages.
Before modeling, the distribution of each outcome variable was examined. Normality was tested using D’Agostino’s K2 test, and dispersion was evaluated by comparing the variance to the mean. All outcomes demonstrated deviation from normality and high right skew with a high frequency of zeros. The variance exceeded the mean and showed overdispersion, which supported the use of negative binomial distribution.
Associations between the proportion of remote consultations and acute mental health service use were estimated using GEEs to account for clustering of patients within GP practices. Negative binomial GEEs were fitted for all four outcomes, including an offset for days at risk to adjust for variation in individual follow-up time. Complete-case analyses were conducted as a sensitivity check. Results are reported as IRRs with 95% CIs.
The proportion of remote consultations during the exposure window was analyzed as a continuous variable and scaled per 10-percentage-point increase. All models were adjusted for demographics (age, sex, ethnicity and IMD decile), clinical history (SMI, anxiety and depression), study subperiod and total GP consultations.
Interactions were tested between consultation modality and age, sex, ethnicity and IMD to examine whether the association between remote care and outcomes differed across demographic groups.
Model fit was assessed using complementary approaches. The QIC was used to compare model structures and optimize the negative binomial dispersion parameter (alpha) for each outcome. Missing data were addressed using MICE, and the impact of imputation on model uncertainty was evaluated using FMI and RIV metrics. Finally, model assumptions were examined using DHARMa-derived QQ plots and residuals-versus-predicted value plots.
All statistical tests were two-sided, and P values <0.05 were considered statistically significant.
Information governance
Data are stored in a third-party database, the Maudsley Biomedical Research Centre CRIS database, which provides access to pseudonymised data derived from source electronic medical records. These data can only be accessed by authorized individuals from within a secure firewall (that is, the data cannot be sent elsewhere).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.