
Midway through the Senate Veterans’ Affairs Committee’s May 20 hearing on the VA’s advance budget request, Sen. Angus King (I-ME) pressed VA Secretary Doug Collins on his view of the future of veterans’ health care. Every net increase in Collins’s FY2028 advance appropriations request was earmarked for care delivered by private-sector providers. To King, the intention seemed unmistakable: a plan “to gradually privatize VA health care coverage.”
Collins’s response was withering in its contempt—for the question and the questioner alike: “There is no intention to gradually, there is no intention to accelerate, there is no intention to decelerate, there is no intention to privatize at all.” Collins also deftly erected a misleading straw man, framing “privatization” as if it means shutting down the Veterans Health Administration (VHA) totally and handing it over to the private sector. As Prospect co-editor Paul Starr explained in a seminal essay, this definition is both misleading and plain wrong, as privatization encompasses any shift of activities, functions, or production of goods from the public sector to the private—including what he calls “privatization by attrition,” in which the expansion of costlier private services starves the public ones of funding. That is precisely what’s been happening—and Collins’s proposed budget would turbocharge it further.
More from Russell Lemle | Suzanne Gordon
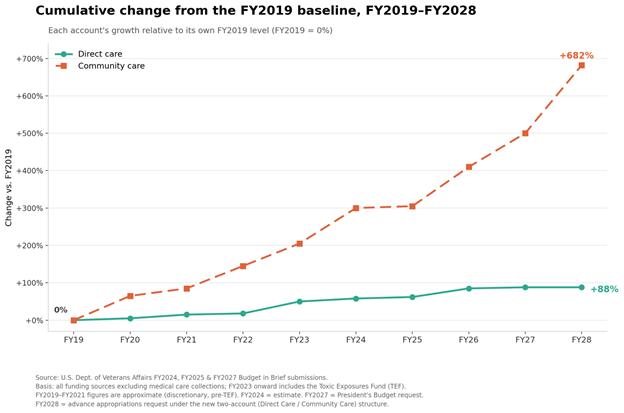
These policies are, of course, the logical extension of the dynamic set in motion a decade ago. The Veterans Choice Program opened veterans’ care to the private sector in 2015; in 2019, it was replaced and expanded by the VA MISSION Act, which mandated the creation of the Veterans Community Care Program (VCCP), a private-sector network that comprises more than 1.7 million providers, including doctors and hospitals. Spending on what has become known as “community care” has gathered momentum every year since, climbing 410 percent above its 2019 level. Over the same period, the VA’s spending on its own direct care rose just 84 percent. Rather than tap the brakes on these runaway community care costs, Collins is flooring the accelerator. By 2028, community care spending will stand at 682 percent above its 2019 level.
By contrast, as Sen. Tammy Duckworth (D-IL)—a disabled veteran and former VA assistant secretary for public and intergovernmental affairs—made clear, Collins’s request for VA in-house care, when adjusted for inflation, represents a cut in the direct care budget, which she called “an abandonment of veterans.” Duckworth also highlighted the discrepancy between Collins’s request and the projections in the Independent Budget (IB), a proposal crafted by two of the largest national veterans service organizations (VSOs): the Disabled American Veterans (DAV) and the Veterans of Foreign Wars (VFW). The IB found that a 19.4 percent increase is needed to keep the VA adequately staffed—the inverse of what Collins is proposing.
Collins responded by deriding the veterans organizations’ projections, shouting at Duckworth that “outside independent agencies are not responsible for anybody. They can put down numbers in any way they want to have it.”
As the two graphs below reveal, the redistribution of veterans health care spending is staggering.
—————
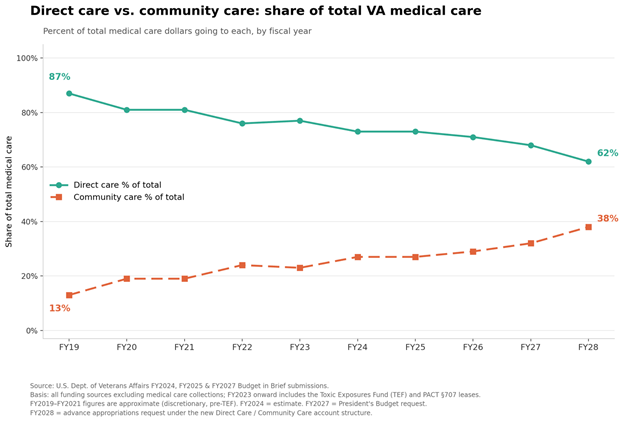
During the hearing, Collins repeatedly insisted that in-house care remains the predominant mode of veterans health care, citing as proof the statistic that the VA spends twice as many dollars on direct care as on community care. That is true—in 2026. But he conveniently ignored the fact that just seven years ago that ratio was 6:1. The trajectory is unambiguous, and Democratic senators are right to recognize that the VA is being privatized in real time. Collins’s denials notwithstanding, we are inexorably approaching the point where more of veterans medical care dollars flow to community providers than to the VA’s own direct care system.
Measured by workload rather than dollars, VCCP is close to surpassing VA—and may already have done so. In FY2023, community care accounted for roughly 40 percent of the total workload volume, and congressional testimony last year by VCCP administrators indicated that share has kept climbing.
Ranking member Richard Blumenthal (D-CT), along with King, questioned Collins about the predictable consequence of eliminating 50,000 VA health care positions, which the Prospect has covered extensively. Blumenthal noted that “failure to properly fund and staff VA health care facilities will force veterans into community care.” For Collins, shrinking the VA’s footprint is not a problem because, he asserted, “the number of employees does not equal success at the VA.” His written testimony went further still, candidly stating that “VHA is assuming that staffing levels will decrease, which is expected to reduce VHA capacity to provide for the growing demand for VA direct care services.” He blithely insisted that no one should fret about how many veterans are sent to the private sector since “community care is VA care,” i.e., veterans receive the same quality from the private sector as from the VA itself.
Countless studies contradict this claim. Care in the community is, on average, both lower in quality and higher in cost than that delivered in the VA.
In a further effort to make the case that care is not being compromised, Collins also invoked the May 18th Centers for Medicare & Medicaid Services hospital quality star ratings, insisting they document the rising quality of VA care amid his workforce reductions. “The Trump Administration has a proven track record of improving Veterans’ care,” he said, “and these ratings underscore that success.” What Collins conveniently omitted was that those CMS ratings are based on data collected between July 2021 and March 2025—a period that falls almost entirely during the Biden administration.
Care Is in Fact Eroding
A variety of surveys and testimonials from VA staff and patients indicate that VA care is eroding as a direct consequence of administration policies.
Take mental health. Since 2020, the number of veterans with a service-connected mental health disability has increased by over 800,000, with no sign of slowing. Post-traumatic stress disorder (PTSD) alone now accounts for more than 1.7 million service-connected veterans. The General Accountability Office reported that demand for mental health appointments is expected to rise 32 percent from 2021 through 2031. Yet Collins is reducing the VA mental health provider workforce. Not surprisingly, VA staff cannot keep pace with demand, and referrals to VCCP mental health providers are surging.
One notable casualty is a program the VA has long held up as a model: team-based Primary Care-Mental Health Integration, or PC-MHI. Unlike most private-sector practices, the VA embeds psychologists or psychiatric nurse practitioners directly in primary care settings. When a patient mentions anxiety or depression to their primary care provider, that provider can walk them down the hall to a mental health clinician on the spot. Studies have consistently found that this model increases access to both initial and ongoing mental health treatment. It depends, however, on having enough staff. Collins’s cuts are dismantling it.
At one East Coast VA health care system, a mental health manager told the Prospect, “They’re just gutting us. Twenty-five social worker and 20 psychologist positions—all in the process of being backfilled last December—were simply wiped off the org chart after Collins’s ceiling caps took effect. Seven of the lost positions were in PC-MHI, even though they are desperately needed.”
According to a chief at another large VA system, staffing cuts and position caps are crippling how mental health services are delivered: “Because of staffing shortages, there is local pressure to make do with fewer staff. The logic is ‘we don’t have enough people, so let’s cut down on the time we give patients to get more people through the door and look good because there are short wait times for appointments.’ It’s not exactly unethical, but it’s not effective, particularly when you’re dealing with serious, chronic mental health problems like PTSD.”
Kayla Williams—an Iraq War veteran and former director of the Center for Women Veterans and assistant secretary for public and intergovernmental affairs at the VA—described the situation firsthand. “My mental health appointments have been cut from 50 minutes to 30 minutes,” she said. “I just spoke to a friend who told me the same thing. She was informed that all her future therapy appointments would only be 30 minutes and wondered how she is going to get anything done in half an hour.”
Facilities are also responding to staffing cuts by mandating truncated courses of treatment. Rather than letting clinical need determine how many sessions a patient receives, administrators are now setting limits on duration. One chief described the situation as an impossible bind. “By capping the number of positions, and shortening the length and number of sessions, leadership is making it totally impossible for us to implement the evidence-based treatment models the VA correctly advised us to follow.”
That’s the case across the board in mental health care. The manager of that East Coast system told the Prospect that severe shortages are decimating the Behavioral Health Interdisciplinary Program (BHIP) teams—the primary vehicle for general mental health care within the VA. The elimination of Community Based Outpatient Clinic therapist positions is pushing more veterans into the private sector.
Another VA source told the Prospect, “PTSD treatment models are designed to help meet what VA has identified as best practice. But we’re not allowed to have the staffing to meet the model. When employees raise concerns about ceiling caps eroding services, national leaders have minimized or dismissed the importance of meeting these models and said explicitly that they are not going to staff to meet the models.”
The problem is so serious that in April the House of Representatives addressed it directly in the report accompanying its Military Construction and Veterans Affairs Appropriations Bill, which passed overwhelmingly. The report expressed concern that certain VA medical centers are “imposing rigid limits on the number or duration of individual psychotherapy sessions in a manner inconsistent with VHA Directive 1160.05, which requires evidence-based, patient-centered care tailored to a Veteran’s individual needs, preferences, and clinical profile.”
VA physicians and other staff are sounding similar alarms. Whistleblowers at the Raymond G. Murphy VA Medical Center in Albuquerque, New Mexico, issued a public “Call to Action” to New Mexico veterans, warning anonymously of “THE SYSTEMIC COLLAPSE OF VETERAN CARE AT THE ALBUQUERQUE VA”—describing a leadership “Culture of Fear” that silences staff, and an “engineered clinical collapse” which prompted surgeons, anesthesiologists, hematologists, and oncologists to resign, causing dangerous delays in care.
Patients, too, are reporting growing difficulty accessing care. In Northern California, Army veteran Chris Bennett has long relied on the VA for treatment of injuries tied to his military service. These include chronic arthritic pain in his wrists and ankles, and headaches, depression, and PTSD stemming from exposure to multiple head injuries. Until recently, Bennett told the Prospect, the VA had been able to care for these problems. “Now,” he says, “it’s almost impossible to get a mental health appointment. When I tried to get a mental health appointment through the VCCP, I couldn’t.”
The staffing crisis is compounded by a potential collapse in physical infrastructure. On the same day as the Senate hearing, the House Veterans’ Affairs Committee took up a slate of bills, including one addressing leasing and infrastructure. The Disabled American Veterans’ witness Jon Retzer testified that the IB analysts—and until recently, the VA’s own projections—had estimated that closing the gap between the system’s aging infrastructure and its needed capacity would require an investment of $85 billion over the next decade. Yet the VA’s most recent budget projection slashed its ten-year construction estimate by two-thirds, to roughly $28 billion. “A reduction of this magnitude in VA’s health care infrastructure could have catastrophic consequences,” Retzer cautioned. “There’s only one way to read this,” one seasoned VSO observer told the Prospect. “The VA intends to downsize its physical facilities.”
In congressional testimony in December 2024, the VFW expressed its own apprehension: “Care in the community is necessary for some veterans but, if given the choice, our members routinely tell us they prefer VA direct care … [The Community Care Network] is a ‘leaking ship,’ and shoving more people onto that ship would be detrimental to those veterans seeking care. We need to plug the holes in this problematic program before unduly adding more veterans to it.”
Veterans don’t want privatization or a VA stripped of its capacity. But without action soon, that may be exactly what they get. Not coincidentally, it would be precisely what the Heritage Foundation’s Project 2025 blueprint prescribed. As Sen. Duckworth stated plainly during the hearing: “Secretary Collins, you have repeatedly denied that Donald Trump wants to privatize the VA to enrich his billionaire donors, but frankly, actions speak louder than words.”
Related